

The distinctive structure and composition of arterial and venous thrombi and pulmonary emboli
- PMID: 32198356
- PMCID: PMC7083848
- DOI: 10.1038/s41598-020-59526-x
The distinctive structure and composition of arterial and venous thrombi and pulmonary emboli
Abstract
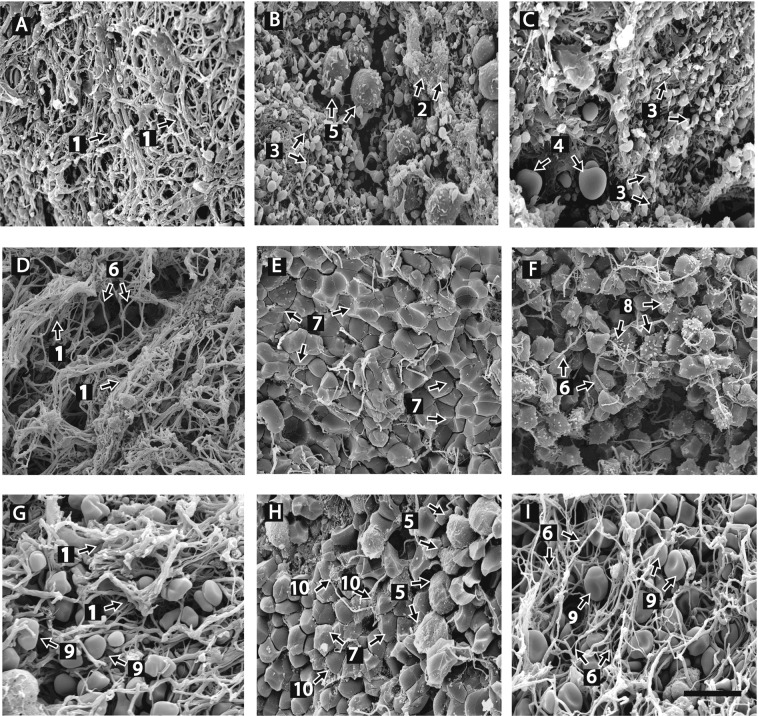
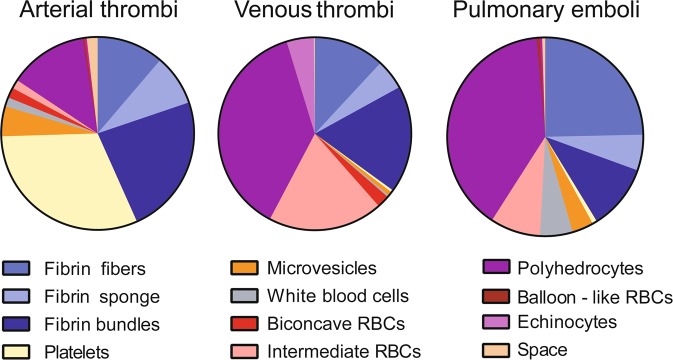
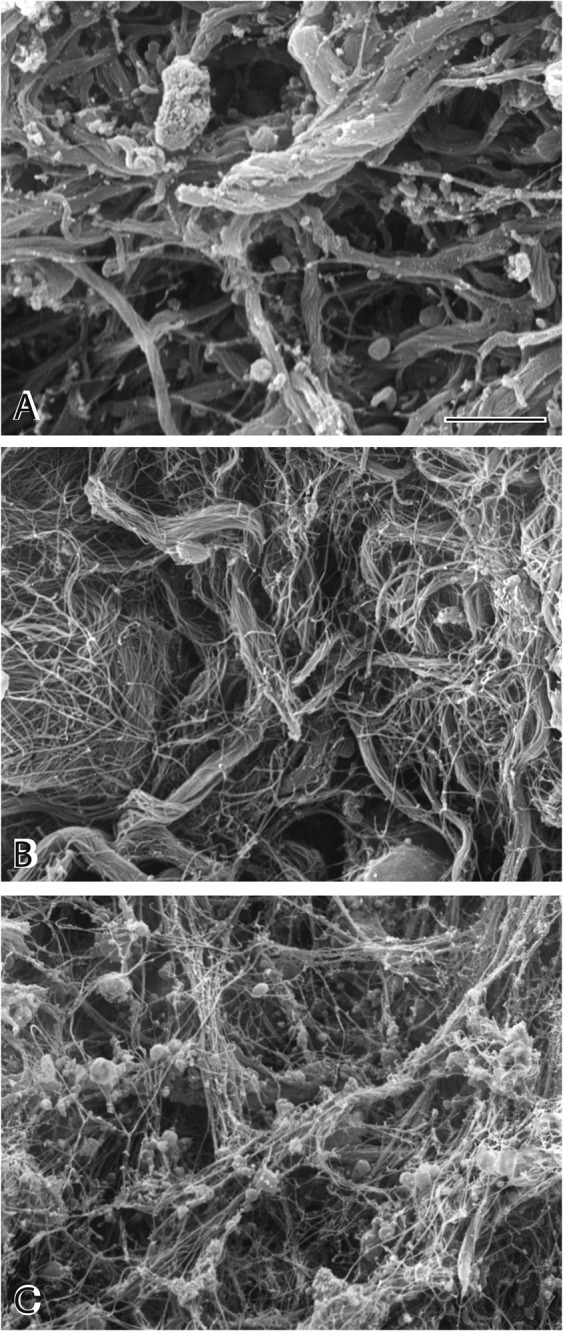
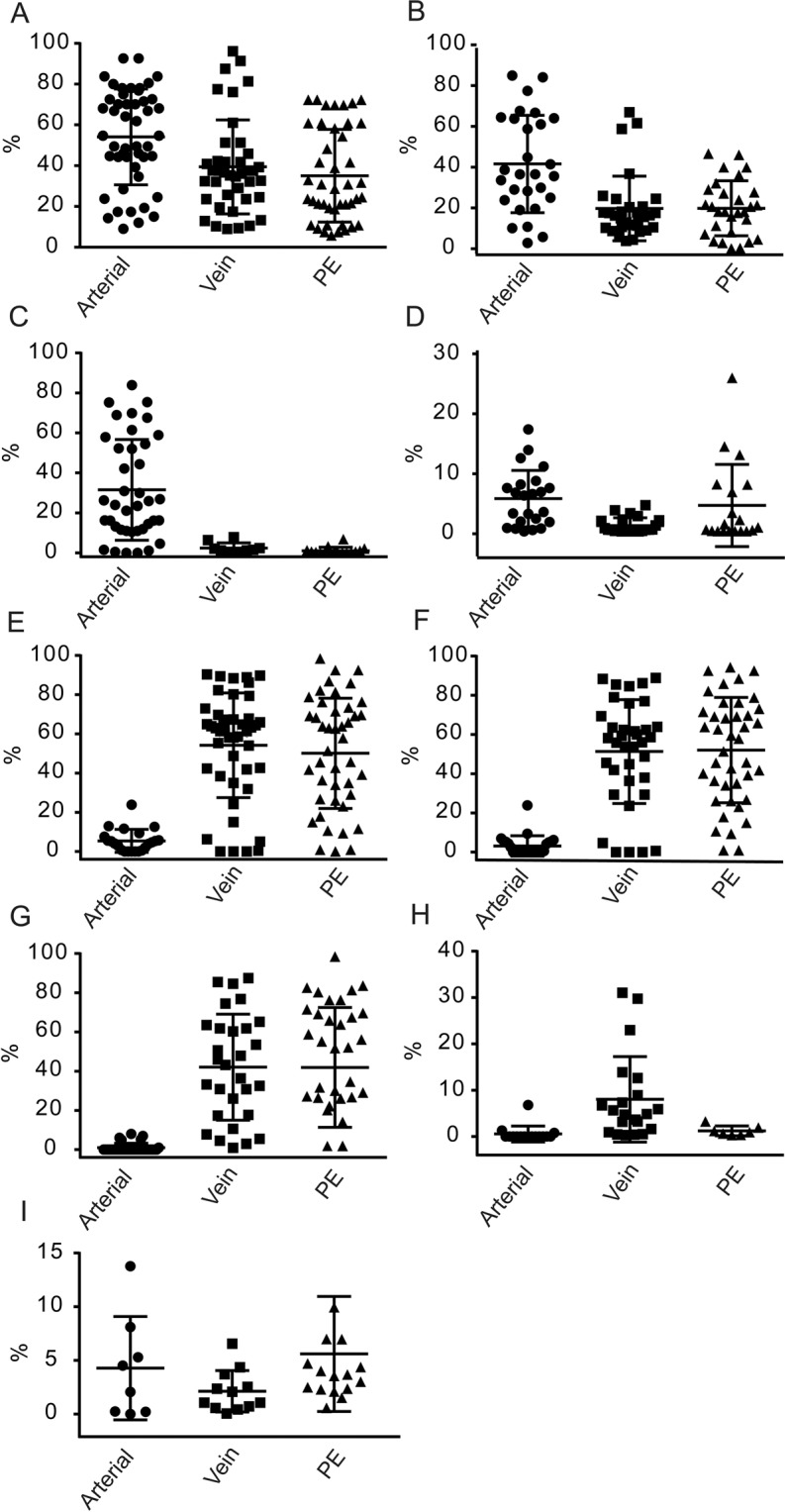
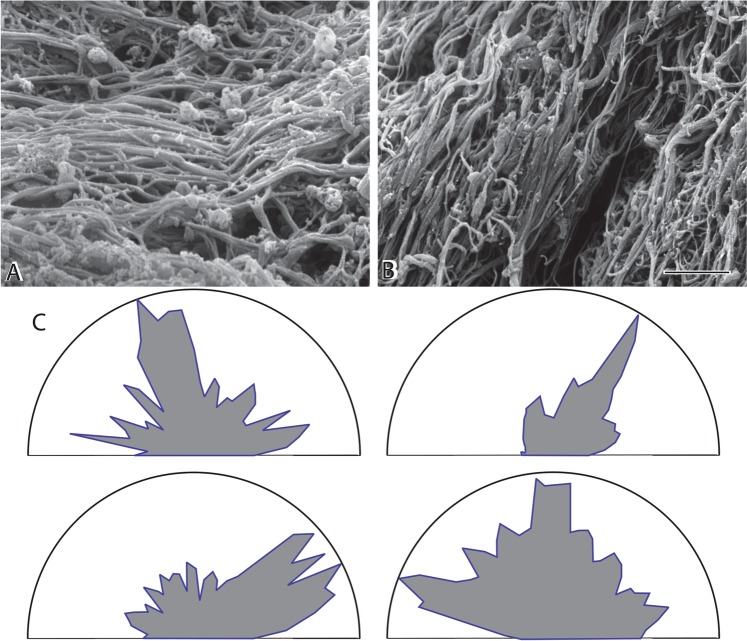
Although arterial and venous thromboembolic disorders are among the most frequent causes of mortality and morbidity, there has been little description of how the composition of thrombi and emboli depends on their vascular origin and age. We quantified the structure and composition of arterial and venous thrombi and pulmonary emboli using high-resolution scanning electron microscopy. Arterial thrombi contained a surprisingly large amount of fibrin, in addition to platelets. The composition of pulmonary emboli mirrored the most distal part of venous thrombi from which they originated, which differed from the structure of the body and head of the same thrombi. All thrombi and emboli contained few biconcave red blood cells but many polyhedrocytes or related forms of compressed red blood cells, demonstrating that these structures are a signature of clot contraction in vivo. Polyhedrocytes and intermediate forms comprised the major constituents of venous thrombi and pulmonary emboli. The structures within all of the thrombi and emboli were very tightly packed, in contrast to clots formed in vitro. There are distinctive, reproducible differences among arterial and venous thrombi and emboli related to their origin, destination and duration, which may have clinical implications for the understanding and treatment of thrombotic disorders.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (In consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996;93:2212–2245. doi: 10.1161/01.CIR.93.12.2212. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
