

A large maxillary cemento-ossifying fibroma superimposed with solitary bone cyst documented over 18 years: A case report
- PMID: 32199251
- PMCID: PMC7082601
- DOI: 10.1016/j.ijscr.2020.03.011
A large maxillary cemento-ossifying fibroma superimposed with solitary bone cyst documented over 18 years: A case report
Abstract
Introduction: Cemento-ossifying fibromas are rare, benign lesions of the head and neck regions. The origin of these lesions can be traced to the periodontal ligament, because its cells are able to form cement, lamellar bone, or fibrous tissue.
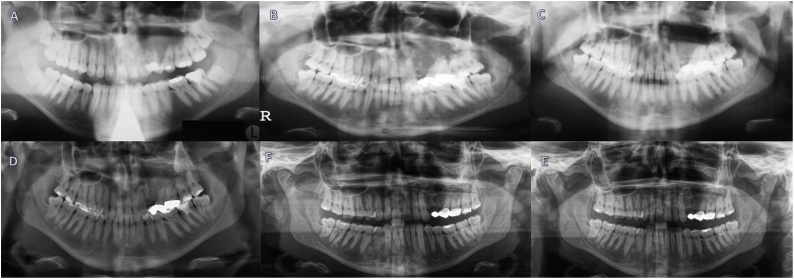
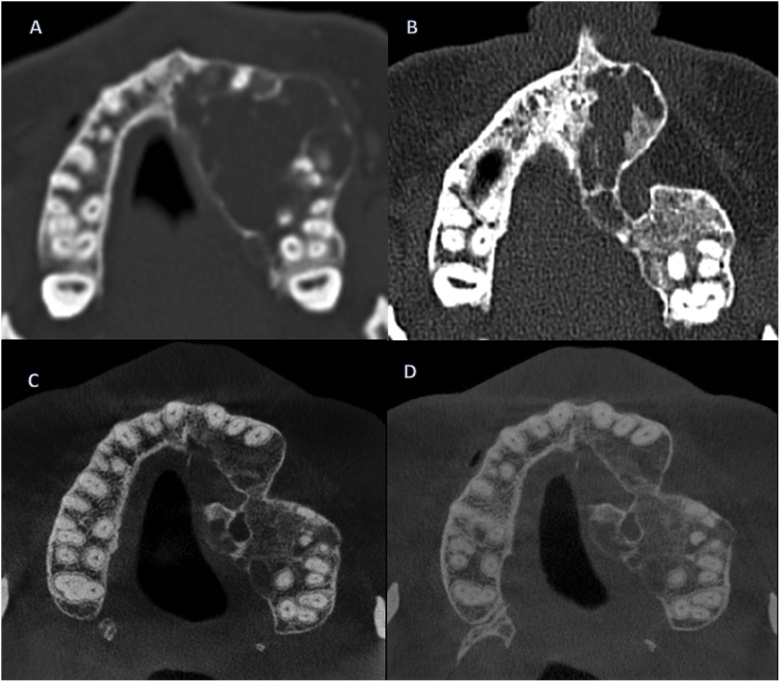
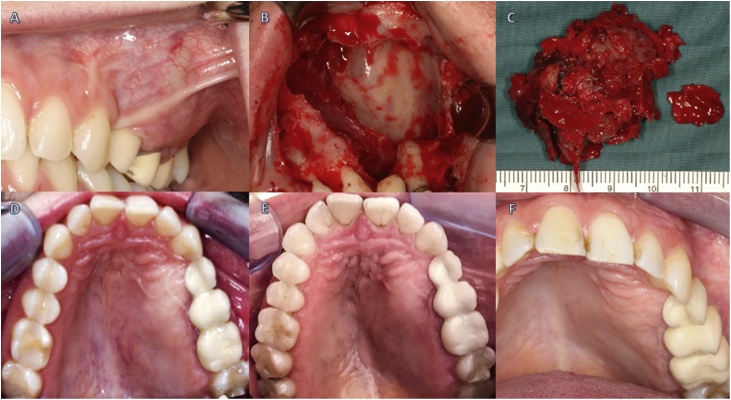
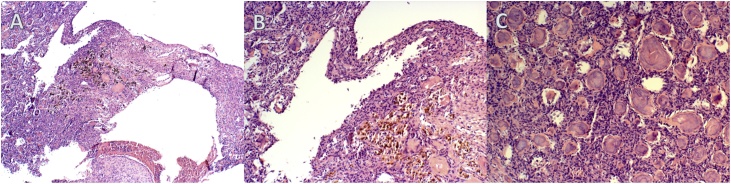
Case presentation: A rare case report of a young Caucasian female with a COF is described including follow-ups. She remained untreated for several years despite early radiographic findings of the lesion without a definitive diagnosis. The patient ultimately underwent radical surgery and the whole lesion was removed. The subsequent histological examination confirmed the clinical diagnosis of a COF. Since then, the patient has been under regular clinical and radiological follow-ups.
Discussion: This rare case report of a COF, documented over 18 years, shows the importance of consecutive therapy after radiologic and clinical findings, as such lesions continue growing and may subsequently lead to severe medical conditions. Therefore, complete surgical resection of COFs is advised to achieve good results in terms of health and recurrence.
Conclusion: Long-term follow-up of patients is required as recurrences can occur for up to 10 years following treatment. Well-planned radical and wide surgical resection of these lesions has proven not only to be effective in eliminating the aetiological factors, but can also achieve decent bone regeneration and aesthetic results with almost no deformation in the surgical site.
Keywords: Case report; Cemento-ossifying fibroma; Fibrous dysplasia; Juvenile ossifying fibroma; Solitary bone cyst.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
Similar articles
-
Ossifying Fibromas of the Head and Neck Region: A Clinicopathological Study of 45 Cases.Head Neck Pathol. 2022 Mar;16(1):248-256. doi: 10.1007/s12105-021-01350-4. Epub 2021 Jun 28. Head Neck Pathol. 2022. PMID: 34184157 Free PMC article.
-
[Multiple cemento-ossifying fibromas of the jaw: a very rare diagnosis].Schweiz Monatsschr Zahnmed. 2007;117(3):236-44. Schweiz Monatsschr Zahnmed. 2007. PMID: 17425241 French, German.
-
Cemento-Ossifying Fibroma in Maxillofacial Region: A Series of 16 Cases.J Maxillofac Oral Surg. 2021 Jun;20(2):240-245. doi: 10.1007/s12663-019-01304-y. Epub 2019 Nov 8. J Maxillofac Oral Surg. 2021. PMID: 33927492 Free PMC article.
-
Cemento-ossifying fibroma of maxillary and sphenoid sinuses: case report and literature review.Acta Otolaryngol Suppl. 2002;(547):118-22. doi: 10.1080/000164802760057734. Acta Otolaryngol Suppl. 2002. PMID: 12212586 Review.
-
Maxillofacial fibro-osseous lesions: classification and differential diagnosis.Semin Diagn Pathol. 1996 May;13(2):104-12. Semin Diagn Pathol. 1996. PMID: 8734416 Review.
Cited by
-
Familial Gigantiform Cementoma with Calcium Steal Phenomenon and Social Stigma: A Case Report with Review of Literature.J Maxillofac Oral Surg. 2022 Dec;21(4):1343-1347. doi: 10.1007/s12663-021-01521-4. Epub 2021 Feb 21. J Maxillofac Oral Surg. 2022. PMID: 36896065 Free PMC article.
References
-
- Tamiolakis D., Thomaidis V., Ioani T. Cementoossifying fibroma of the maxilla: a case report. Acta Stomatol. Croat. 2005;39(3):319–321.
-
- Bertrand B., Eloy Ph., Cornelis J.P.H., Gosseye S., Clotuche J., Gilliard C.L. Juvenile aggressive cemento-ossifying fibroma: case report and review of the literature. Laryngoscope. 1993;103(12):1321–1448. - PubMed
-
- Hamner J.E., Scofield H.H., Col J.C.L. Benign fibro‐osseous jaw lesions of periodontal membrane origin. An analysis of 249 cases. Cancer. 1968;22(4):861–878. - PubMed
-
- Blayney A., Tayeb A. The ‘hybrid’ fibro-osseous lesion. J. Laryngol. Otol. 1986;100(3):291–302. - PubMed
-
- Su L., Weathers D., Waldron C. Distinguishing features of focal cemento-osseous dysplasia and cemento-ossifying fibromas. II. A clinical and radiologic spectrum of 316 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997;84(540–549) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
