

The risk of tuberculosis in children after close exposure: a systematic review and individual-participant meta-analysis
- PMID: 32199484
- PMCID: PMC7289654
- DOI: 10.1016/S0140-6736(20)30166-5
The risk of tuberculosis in children after close exposure: a systematic review and individual-participant meta-analysis
Abstract
Background: Tens of millions of children are exposed to Mycobacterium tuberculosis globally every year; however, there are no contemporary estimates of the risk of developing tuberculosis in exposed children. The effectiveness of contact investigations and preventive therapy remains poorly understood.
Methods: In this systematic review and meta-analysis, we investigated the development of tuberculosis in children closely exposed to a tuberculosis case and followed for incident disease. We restricted our search to cohort studies published between Jan 1, 1998, and April 6, 2018, in MEDLINE, Web of Science, BIOSIS, and Embase electronic databases. Individual-participant data and a pre-specified list of variables were requested from authors of all eligible studies. These included characteristics of the exposed child, the index case, and environmental characteristics. To be eligible for inclusion in the final analysis, a dataset needed to include: (1) individuals below 19 years of age; (2) follow-up for tuberculosis for a minimum of 6 months; (3) individuals with household or close exposure to an individual with tuberculosis; (4) information on the age and sex of the child; and (5) start and end follow-up dates. Studies assessing incident tuberculosis but without dates or time of follow-up were excluded. Our analysis had two primary aims: (1) estimating the risk of developing tuberculosis by time-period of follow-up, demographics (age, region), and clinical attributes (HIV, tuberculosis infection status, previous tuberculosis); and (2) estimating the effectiveness of preventive therapy and BCG vaccination on the risk of developing tuberculosis. We estimated the odds of prevalent tuberculosis with mixed-effects logistic models and estimated adjusted hazard ratios (HRs) for incident tuberculosis with mixed-effects Poisson regression models. The effectiveness of preventive therapy against incident tuberculosis was estimated through propensity score matching. The study protocol is registered with PROSPERO (CRD42018087022).
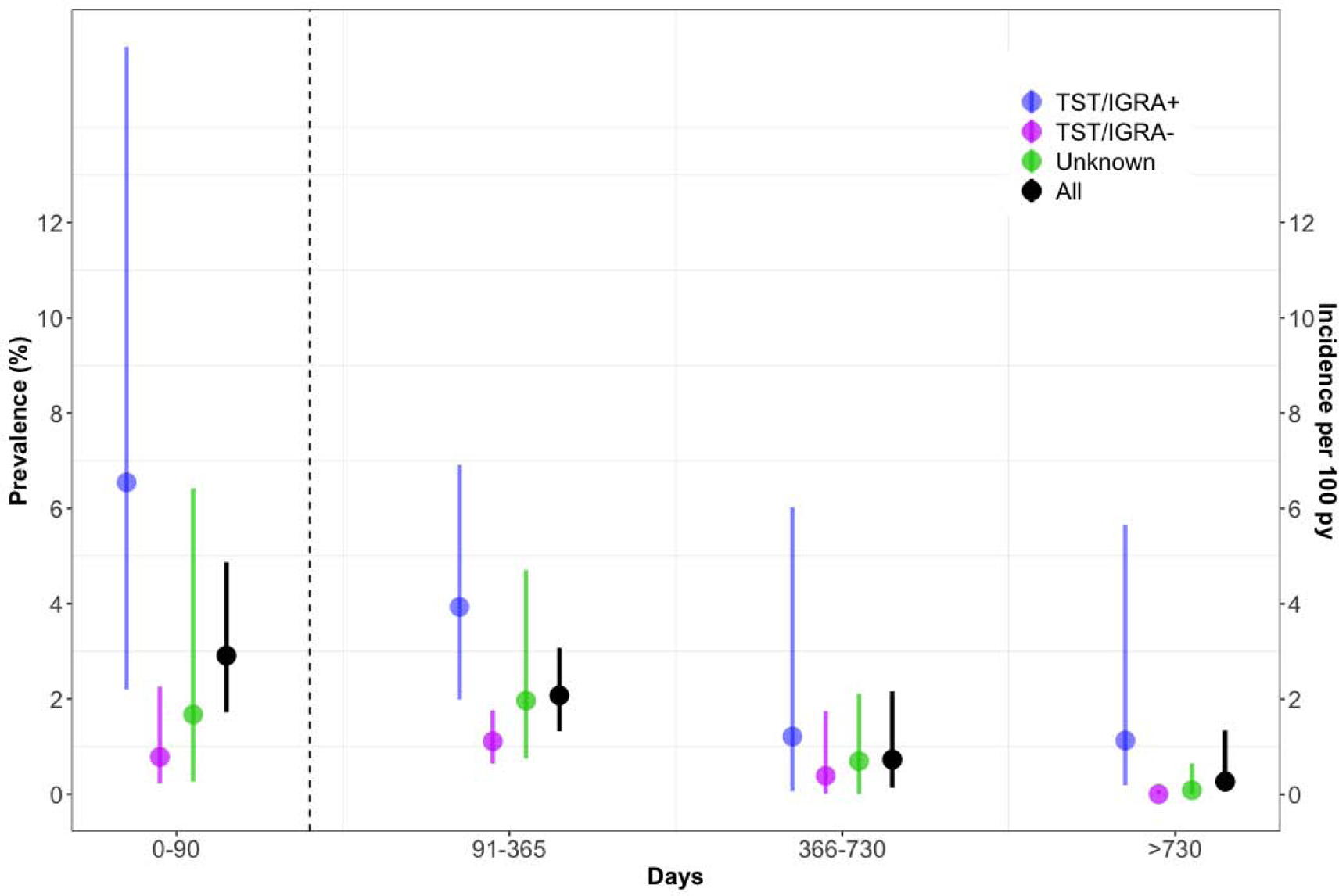
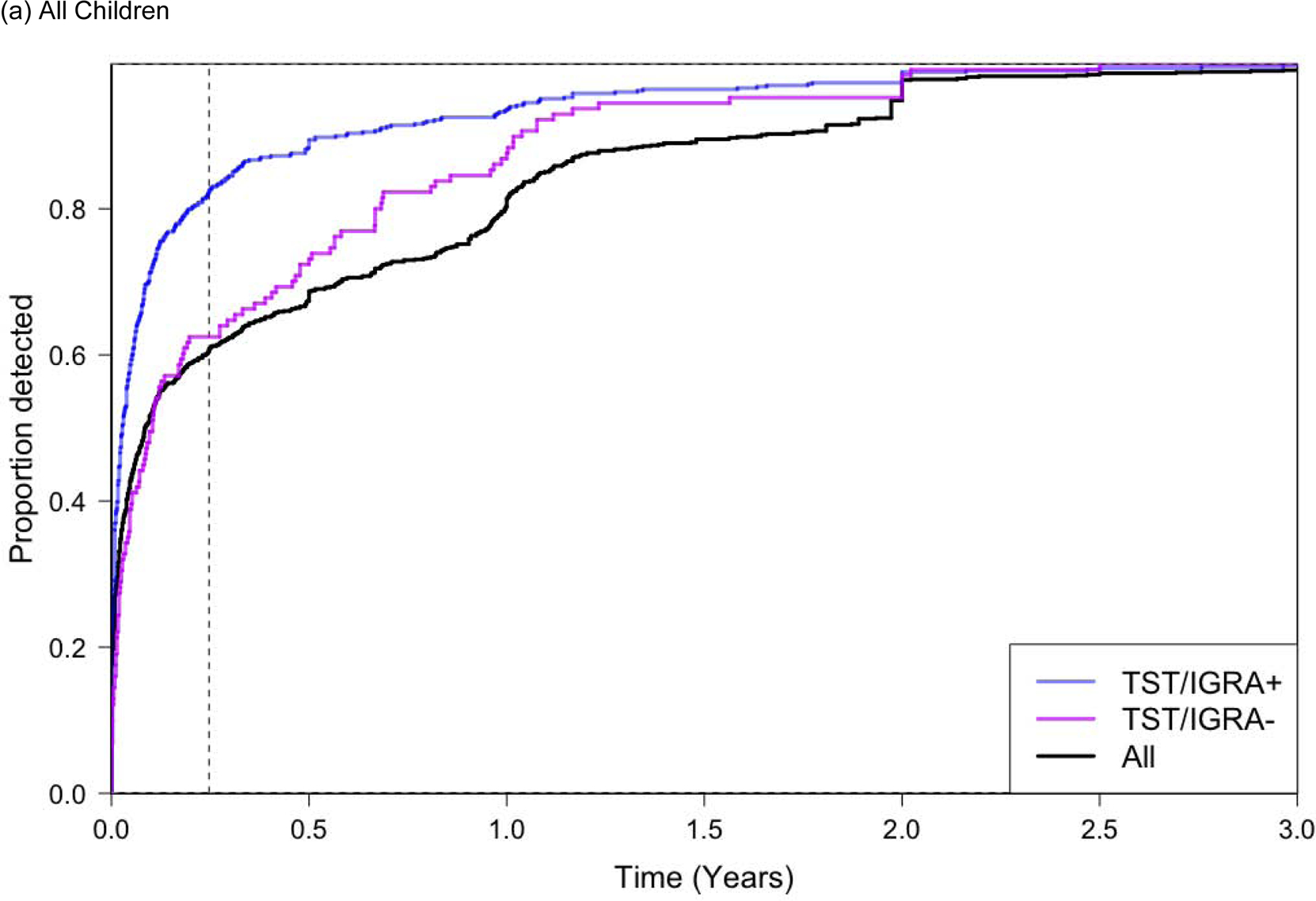
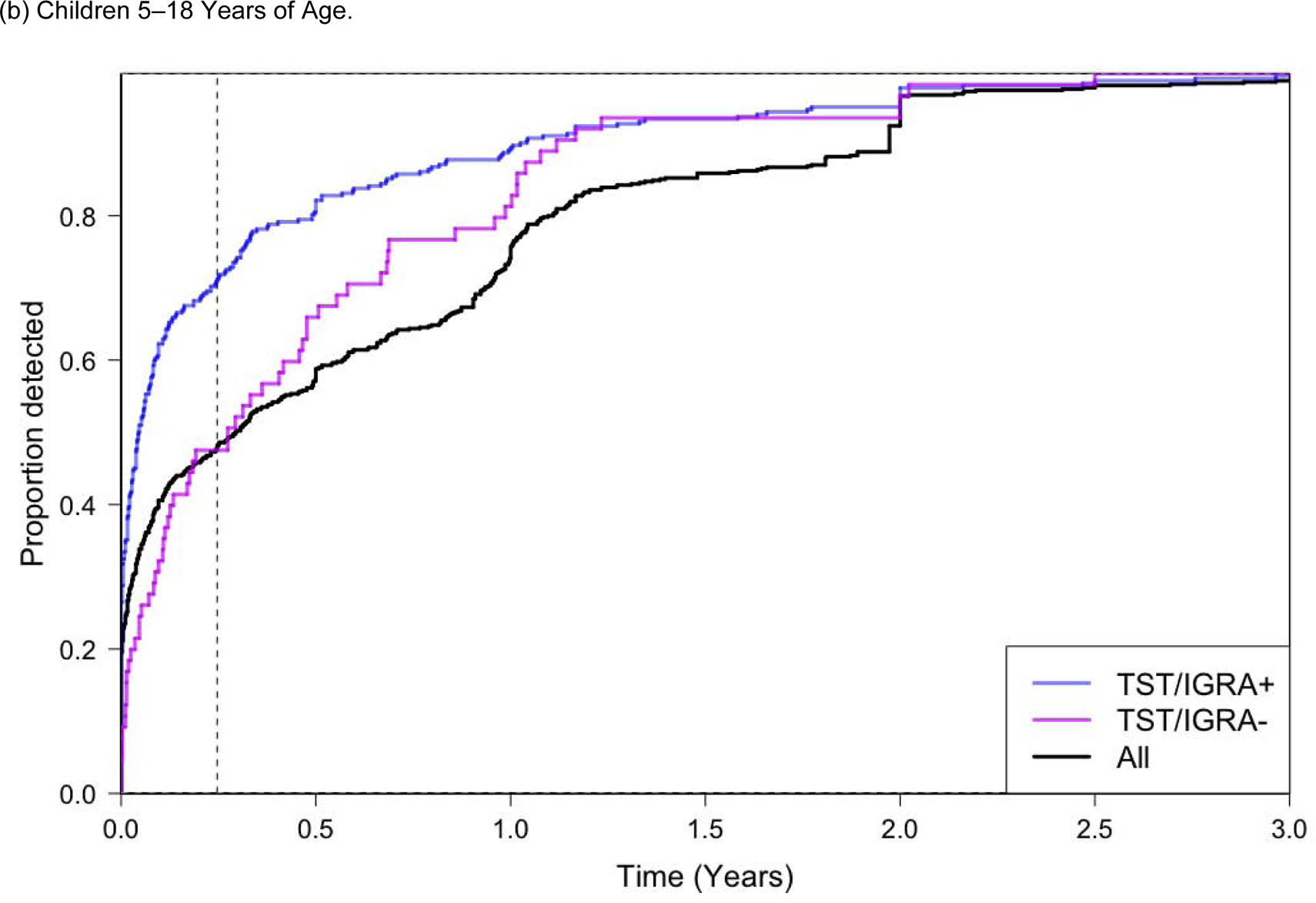
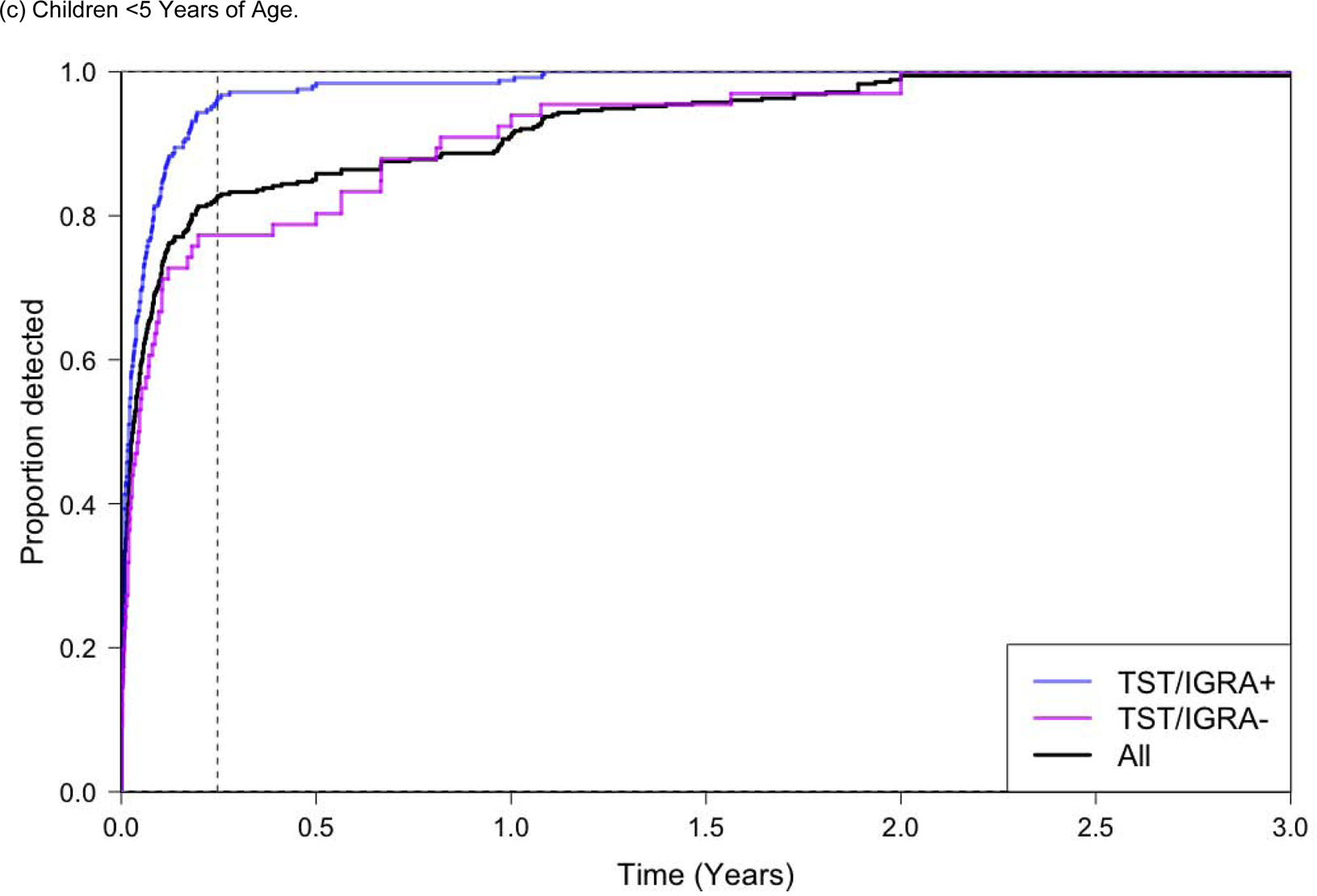
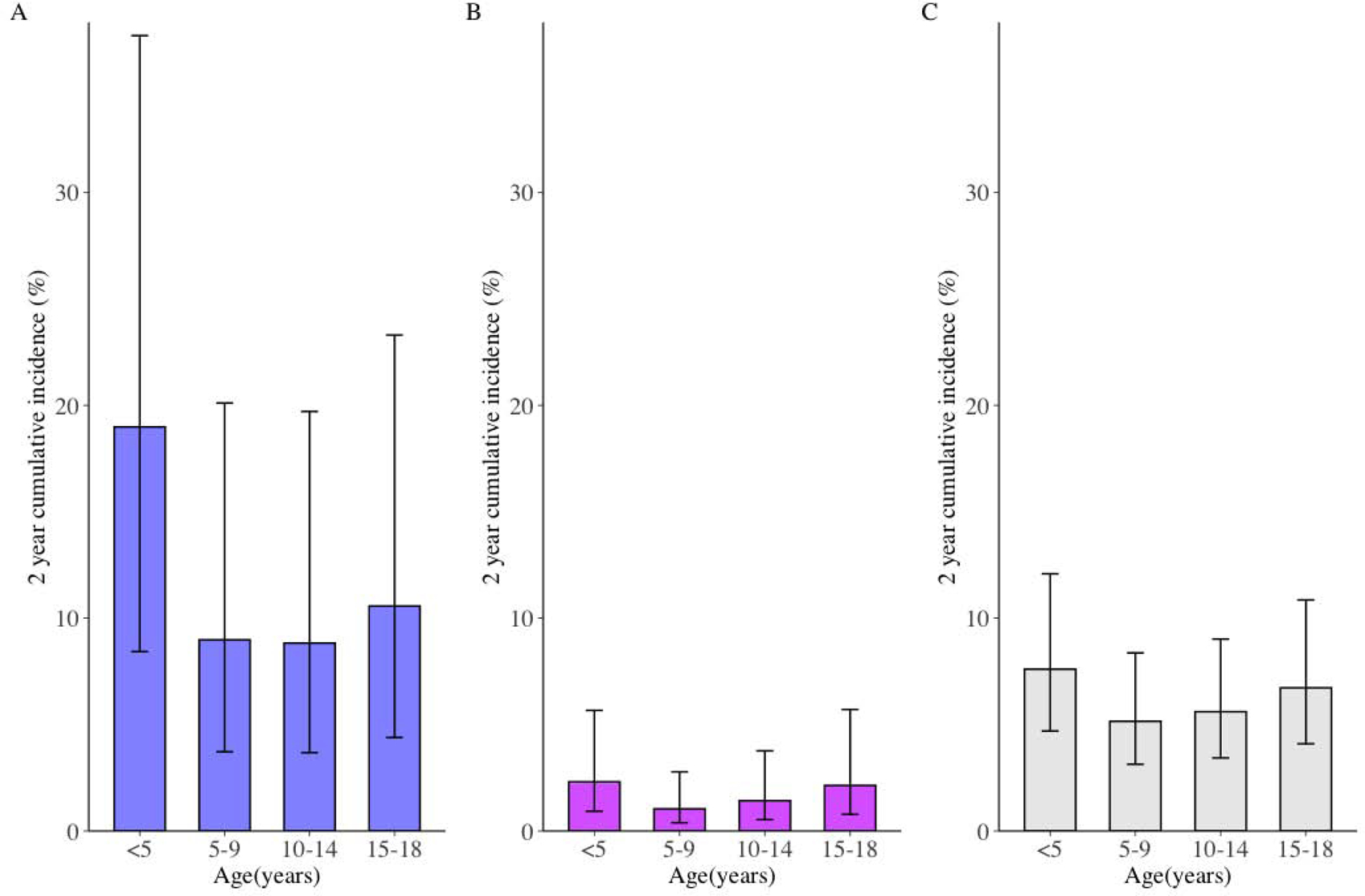
Findings: In total, study groups from 46 cohort studies in 34 countries-29 (63%) prospective studies and 17 (37%) retrospective-agreed to share their data and were included in the final analysis. 137 647 tuberculosis-exposed children were evaluated at baseline and 130 512 children were followed for 429 538 person-years, during which 1299 prevalent and 999 incident tuberculosis cases were diagnosed. Children not receiving preventive therapy with a positive result for tuberculosis infection had significantly higher 2-year cumulative tuberculosis incidence than children with a negative result for tuberculosis infection, and this incidence was greatest among children below 5 years of age (19·0% [95% CI 8·4-37·4]). The effectiveness of preventive therapy was 63% (adjusted HR 0·37 [95% CI 0·30-0·47]) among all exposed children, and 91% (adjusted HR 0·09 [0·05-0·15]) among those with a positive result for tuberculosis infection. Among all children <5 years of age who developed tuberculosis, 83% were diagnosed within 90 days of the baseline visit.
Interpretation: The risk of developing tuberculosis among exposed infants and young children is very high. Most cases occurred within weeks of contact investigation initiation and might not be preventable through prophylaxis. This suggests that alternative strategies for prevention are needed, such as earlier initiation of preventive therapy through rapid diagnosis of adult cases or community-wide screening approaches.
Funding: National Institutes of Health.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
No time to waste: preventing tuberculosis in children.Lancet. 2020 Mar 21;395(10228):924-926. doi: 10.1016/S0140-6736(20)30532-8. Lancet. 2020. PMID: 32199475 No abstract available.
References
-
- Dodd PJ, Gardiner E, Coghlan R and Seddon JA, 2014. Burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. The lancet global health, 2(8), pp. e453–e459. - PubMed
-
- Dodd PJ, Sismanidis C and Seddon JA, 2016. Global burden of drug-resistant tuberculosis in children: a mathematical modelling study. The Lancet infectious diseases, 16(10), pp.1193–1201. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
