

Left Ventricular Remodeling After Transcatheter Versus Surgical Therapy in Adults With Coarctation of Aorta
- PMID: 32199847
- PMCID: PMC7486991
- DOI: 10.1016/j.jcmg.2020.01.016
Left Ventricular Remodeling After Transcatheter Versus Surgical Therapy in Adults With Coarctation of Aorta
Abstract
Objectives: The purpose of this retrospective cohort study was to compare remodeling of left ventricular (LV) structure and function after transcatheter stent therapy with remodeling of LV structure and function after surgical therapy for COA.
Background: Transcatheter stent therapy is as effective as surgery in producing acute hemodynamic improvement in patients with coarctation of aorta (COA). However, LV remodeling after transcatheter COA intervention has not been systematically investigated.
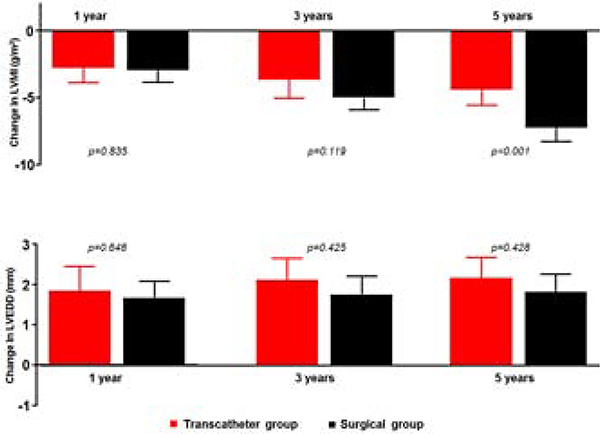
Methods: LV remodeling was assessed at 1, 3, and 5 years post-intervention by using LV mass index (LVMI), LV end-diastolic dimension, LV ejection fraction, LV global longitudinal strain (LVGLS), LV mitral annular tissue Doppler early velocity (LVe'), and ratio of mitral inflow pulsed wave Doppler early velocity and e' (E/e') ratio.
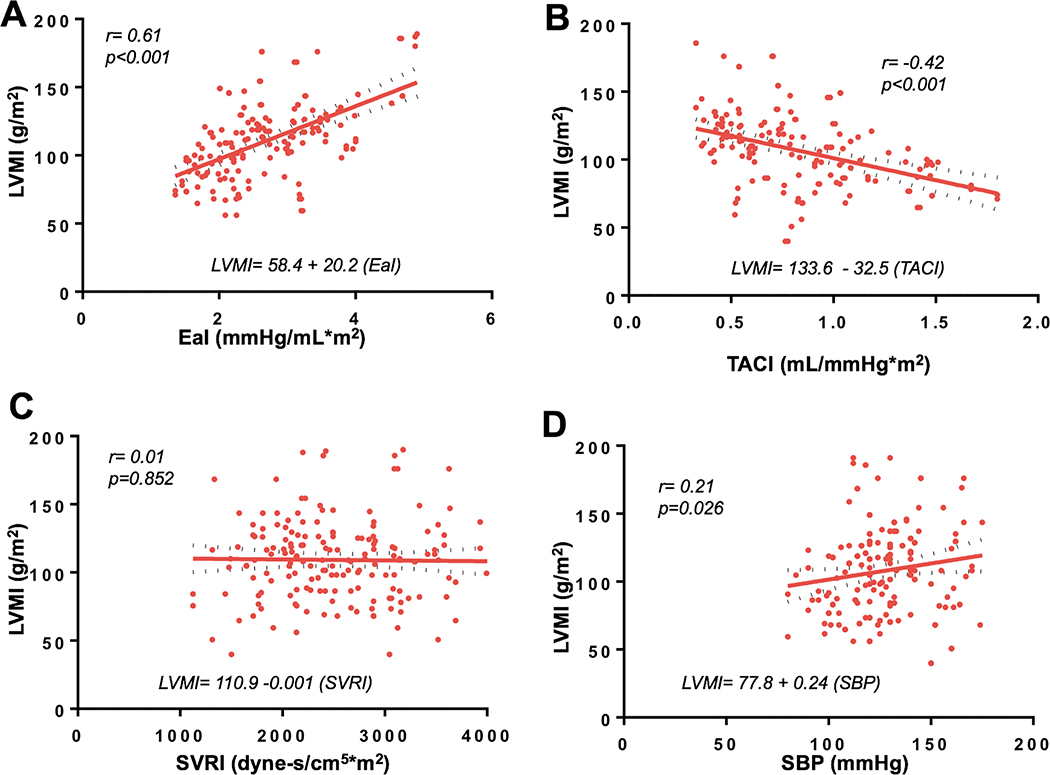
Results: There were 44 patients in the transcatheter group and 128 patients in the surgical group. Compared to the surgical group, the transcatheter group had less regression of LVMI (-4.6; 95% confidence interval [CI]: -5.5 to -3.7 vs. -7.3; 95% CI: -8.4 to -6.6 g/m2; p < 0.001), less improvement in LVGLS (2.1; 95% CI: 1.8 to 2.4 vs. 2.9; 95% CI: 2.6 to 3.2%; p = 0.024), and in e' (1.0 ; 95% CI: 0.7 to 1.2 vs. 1.5 ; 95% CI: 1.3 to 1.7 cm/s; p = 0.009) at 5 years post-intervention. Exploratory analysis showed a correlation between change in LVMI and LVGLS, and between change in LVMI and mitral annular tissue Doppler early velocity (e'), and this correlations were independent of the type of intervention received.
Conclusions: Transcatheter stent therapy was associated with less remodeling of LV structure and function during mid-term follow-up. As transcatheter stent therapy becomes more widely used in the adult COA population, there is a need for ongoing clinical monitoring to determine if these observed differences in LV remodeling translate to differences in clinical outcomes.
Keywords: coarctation of aorta; left ventricular hypertrophy; left ventricular remodeling; transcatheter stent therapy.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Does Surgical Treatment of Coarctation in Adults Result in Better Outcomes Compared With the Transcatheter Approach?JACC Cardiovasc Imaging. 2020 Sep;13(9):1873-1874. doi: 10.1016/j.jcmg.2020.05.020. JACC Cardiovasc Imaging. 2020. PMID: 32912471 No abstract available.
Similar articles
-
Predictors of left ventricular reverse remodelling after coarctation of aorta intervention.Eur Heart J Cardiovasc Imaging. 2021 Sep 20;22(10):1168-1173. doi: 10.1093/ehjci/jeaa199. Eur Heart J Cardiovasc Imaging. 2021. PMID: 33020809 Free PMC article.
-
Left ventricular adaptation to aortic regurgitation in adults with repaired coarctation of aorta.Int J Cardiol. 2023 Jul 15;383:62-69. doi: 10.1016/j.ijcard.2023.04.061. Epub 2023 May 4. Int J Cardiol. 2023. PMID: 37149005
-
[Effect of positive end-expiratory pressure on cardiac function in patients with early left ventricular diastolic dysfunction: a prospective cohort study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Oct;34(10):1066-1071. doi: 10.3760/cma.j.cn121430-20220414-00369. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36473565 Chinese.
-
Increased prevalence of left ventricular diastolic dysfunction in adults with repaired coarctation of aorta.Int J Cardiol Heart Vasc. 2020 May 18;28:100530. doi: 10.1016/j.ijcha.2020.100530. eCollection 2020 Jun. Int J Cardiol Heart Vasc. 2020. PMID: 32462075 Free PMC article.
-
Determinants of Left Ventricular Diastolic Function and Exertional Symptoms in Adults With Coarctation of Aorta.Circ Heart Fail. 2020 Feb;13(2):e006651. doi: 10.1161/CIRCHEARTFAILURE.119.006651. Epub 2020 Feb 14. Circ Heart Fail. 2020. PMID: 32059629 Free PMC article.
Cited by
-
Four-Dimensional flow Magnetic Resonance Imaging for Assessment of Pediatric Coarctation of the Aorta.J Magn Reson Imaging. 2022 Jan;55(1):200-208. doi: 10.1002/jmri.27802. Epub 2021 Jun 26. J Magn Reson Imaging. 2022. PMID: 34173693 Free PMC article.
-
Hemodynamics and Clinical Implications of Occult Left Ventricular Dysfunction in Adults Undergoing Ebstein Anomaly Repair.Circ Cardiovasc Imaging. 2021 Feb;14(2):e011739. doi: 10.1161/CIRCIMAGING.120.011739. Epub 2021 Feb 15. Circ Cardiovasc Imaging. 2021. PMID: 33583197 Free PMC article.
-
Incidence and Outcomes of Advanced Heart Failure in Adults With Congenital Heart Disease.Circ Heart Fail. 2022 Dec;15(12):e009675. doi: 10.1161/CIRCHEARTFAILURE.122.009675. Epub 2022 Oct 4. Circ Heart Fail. 2022. PMID: 36193744 Free PMC article.
-
Prognostic Value of the Anatomic-Physiologic Classification in Adults With Congenital Heart Disease.Circ Heart Fail. 2023 Sep;16(9):e010404. doi: 10.1161/CIRCHEARTFAILURE.122.010404. Epub 2023 Jul 21. Circ Heart Fail. 2023. PMID: 37476989 Free PMC article.
-
Assessment of Coarctation of Aorta Gradient: Echocardiogram-Catheterization Correlation.Am J Cardiol. 2023 Oct 15;205:420-421. doi: 10.1016/j.amjcard.2023.08.083. Epub 2023 Sep 1. Am J Cardiol. 2023. PMID: 37660667 Free PMC article. No abstract available.
References
-
- Zomer AC, Vaartjes I, van der Velde ET, et al. Heart failure admissions in adults with congenital heart disease; risk factors and prognosis. International journal of cardiology. 2013;168:2487–93. - PubMed
-
- Brown ML, Burkhart HM, Connolly HM, et al. Coarctation of the aorta: lifelong surveillance is mandatory following surgical repair. Journal of the American College of Cardiology. 2013;62:1020–5. - PubMed
-
- Rinnstrom D, Dellborg M, Thilen U, et al. Left ventricular hypertrophy in adults with previous repair of coarctation of the aorta; association with systolic blood pressure in the high normal range. International journal of cardiology. 2016;218:59–64. - PubMed
-
- Lombardi KC, Northrup V, McNamara RL, Sugeng L and Weismann CG. Aortic stiffness and left ventricular diastolic function in children following early repair of aortic coarctation. The American journal of cardiology. 2013;112:1828–33. - PubMed
-
- de Divitiis M, Pilla C, Kattenhorn M, et al. Ambulatory blood pressure, left ventricular mass, and conduit artery function late after successful repair of coarctation of the aorta. Journal of the American College of Cardiology. 2003;41:2259–2265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
