

Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis
- PMID: 32199915
- PMCID: PMC7293940
- DOI: 10.1016/j.euo.2020.02.007
Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis
Erratum in
-
Corrigendum to 'Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis' [European Urology Oncology 3 (2020) 306-315].Eur Urol Oncol. 2020 Dec;3(6):811. doi: 10.1016/j.euo.2020.10.003. Epub 2020 Oct 22. Eur Urol Oncol. 2020. PMID: 33575545 Free PMC article.
-
Corrigendum to 'Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis' [European Urology Oncology 3 (2020) 306-315].Eur Urol Oncol. 2020 Oct 21:S2588-9311(20)30168-1. doi: 10.1016/j.euo.2020.10.003. Online ahead of print. Eur Urol Oncol. 2020. PMID: 34756363 No abstract available.
Abstract
Context: A noninvasive multiparametric magnetic resonance imaging (MRI)-based scoring system for predicting muscle-invasive bladder cancer (MIBC), the "Vesical Imaging Reporting and Data System" (VI-RADS), was recently developed by an international multidisciplinary panel. Since then, a few studies evaluating the value of VI-RADS for predicting MIBC have been published.
Objective: To review the diagnostic performance of VI-RADS for the prediction of MIBC.
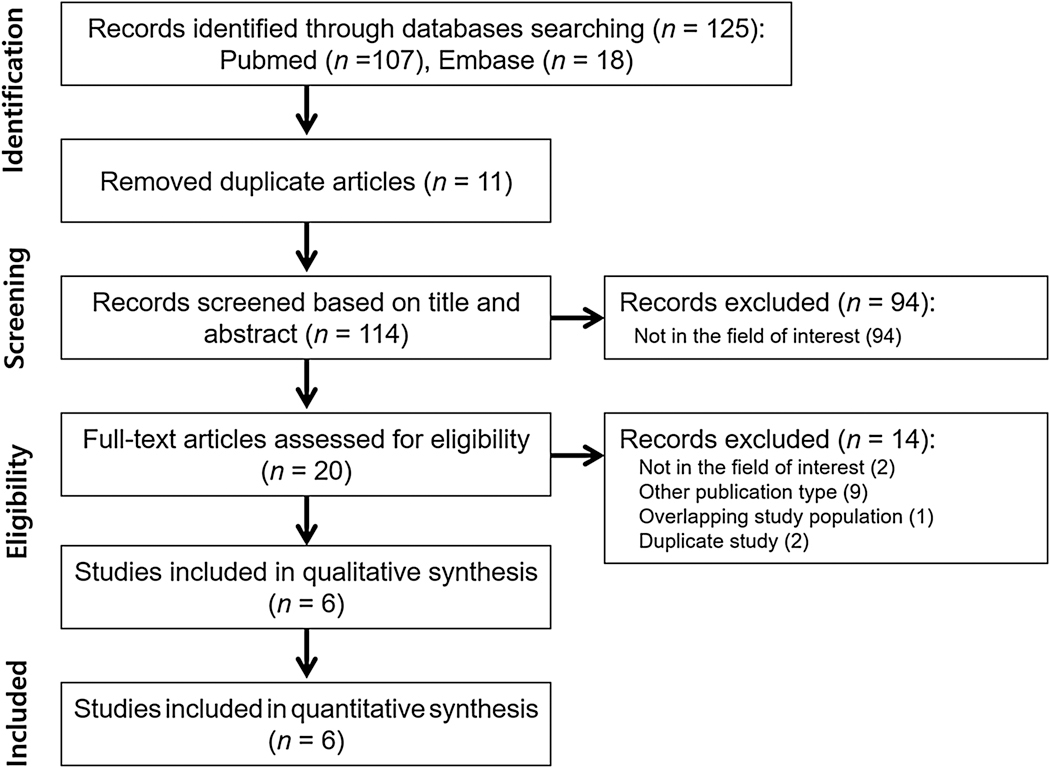
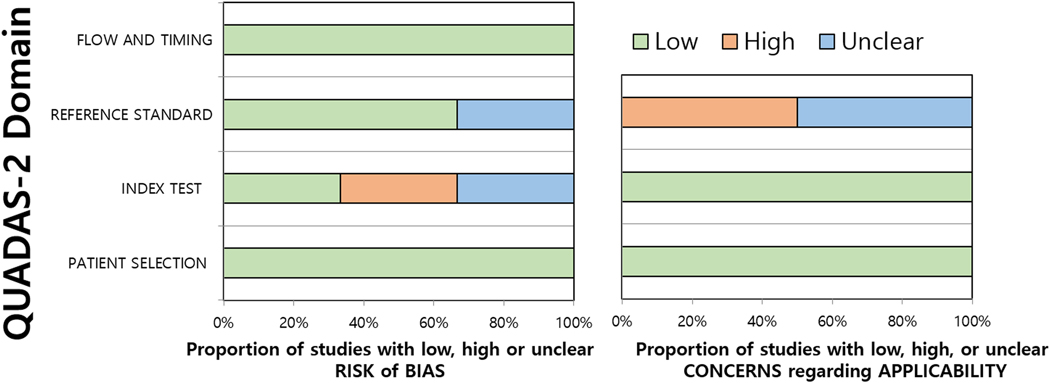
Evidence acquisition: PubMed and EMBASE databases were searched up to November 10, 2019. We included diagnostic accuracy studies using VI-RADS to predict MIBC using cystectomy or transurethral resection as the reference standard. Methodological quality was evaluated with Quality Assessment of Diagnostic Accuracy Studies-2. Sensitivity and specificity were pooled and plotted using hierarchical summary receiver operating characteristics (HSROC) modeling. Meta-regression analyses were done to explore heterogeneity.
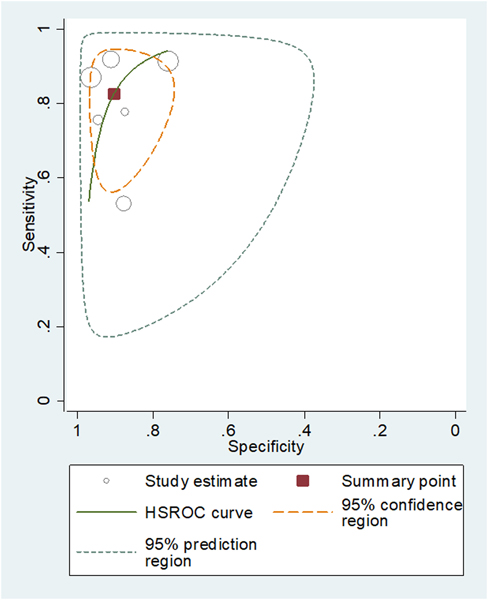
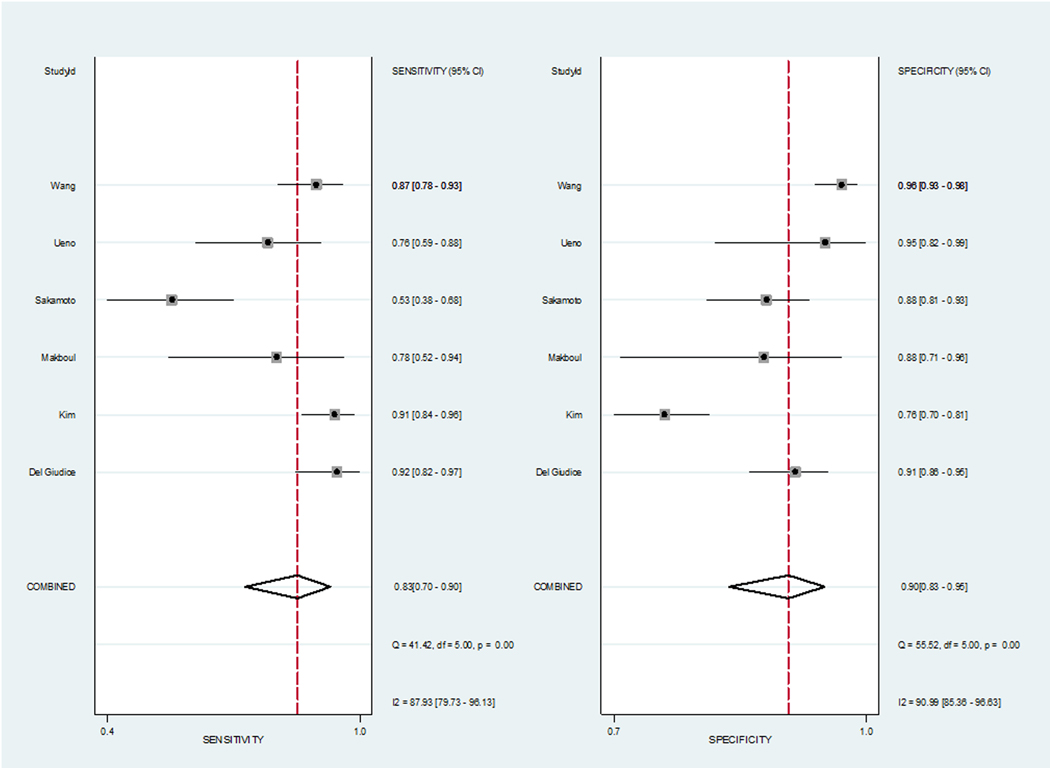
Evidence synthesis: Six studies (1770 patients) were included. Pooled sensitivity and specificity were 0.83 (95% confidence interval [CI] 0.70-0.90) and 0.90 (95% CI 0.83-0.95), and the area under the HSROC curve was 0.94 (95% CI 0.91-0.95). Heterogeneity was present among the studies (Q = 29.442, p < 0.01; I2 = 87.93%, and 90.99% for sensitivity and specificity). Meta-regression analyses showed that the number of patients (>205 vs ≤205), magnetic field strength (3 vs 1.5 T), T2-weighted image slice thickness (3 vs 4 mm), and VI-RADS cutoff score (≥3 vs ≥4) were significant factors affecting heterogeneity (p ≤ 0.03).
Conclusions: VI-RADS shows good sensitivity and specificity for determining MIBC. Technical factors associated with MRI acquisition and cutoff scores need to be taken into consideration as they may affect performance.
Patient summary: A recently established noninvasive magnetic resonance imaging-based scoring system shows good diagnostic performance in detecting muscle-invasive bladder cancer.
Keywords: Bladder cancer; Magnetic resonance imaging; Meta-analysis; Muscle invasive; Systematic review; Vesical Imaging Reporting and Data System.
Copyright © 2020 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Vesical Imaging-Reporting and Data System (VI-RADS) for Bladder Cancer Diagnostics: The Replacement for Surgery?Eur Urol Oncol. 2020 Jun;3(3):316-317. doi: 10.1016/j.euo.2020.03.001. Epub 2020 Apr 14. Eur Urol Oncol. 2020. PMID: 32303479 No abstract available.
-
Re: Sungmin Woo, Valeria Panebianco, Yoshifumi Narumi, Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis. Eur Urol Oncol 2020;3:306-315.Eur Urol Oncol. 2020 Aug;3(4):555-556. doi: 10.1016/j.euo.2020.05.005. Epub 2020 Jun 11. Eur Urol Oncol. 2020. PMID: 32536572 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Josephson D, Pasin E, Stein JP. Superficial bladder cancer: part 2. Management. Expert Rev Anticancer Ther 2007;7:567–81. - PubMed
-
- Chang SS, Boorjian SA, Chou R, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J Urol 2016;196:1021–9. - PubMed
-
- Babjuk M, Burger M, Comperat EM, et al. European Association of Urology guidelines on non-muscle- invasive bladder cancer (TaT1 and carcinoma in situ)—2019 update. Eur Urol 2019;76:639–57. - PubMed
-
- Naselli A, Hurle R, Paparella S, et al. Role of restaging transurethral resection for T1 non–muscle invasive bladder cancer: a systematic review and meta-analysis. Eur Urol Focus 2018;4:558–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
