

What the percentage of births in facilities does not measure: readiness for emergency obstetric care and referral in Senegal
- PMID: 32201621
- PMCID: PMC7059423
- DOI: 10.1136/bmjgh-2019-001915
What the percentage of births in facilities does not measure: readiness for emergency obstetric care and referral in Senegal
Abstract
Introduction: Increases in facility deliveries in sub-Saharan Africa have not yielded expected declines in maternal mortality, raising concerns about the quality of care provided in facilities. The readiness of facilities at different health system levels to provide both emergency obstetric and newborn care (EmONC) as well as referral is unknown. We describe this combined readiness by facility level and region in Senegal.
Methods: For this cross-sectional study, we used data from nine Demographic and Health Surveys between 1992 and 2017 in Senegal to describe trends in location of births over time. We used data from the 2017 Service Provision Assessment to describe EmONC and emergency referral readiness across facility levels in the public system, where 94% of facility births occur. A national global positioning system facility census was used to map access from lower-level facilities to the nearest facility performing caesareans.
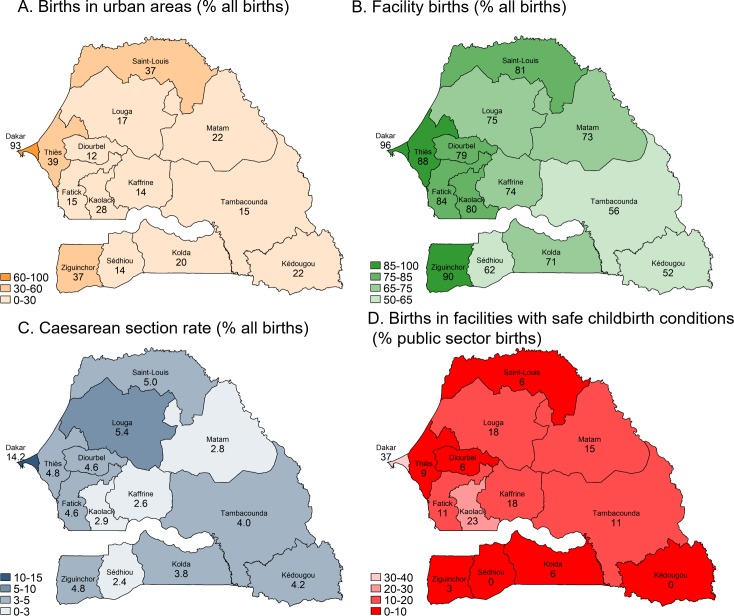
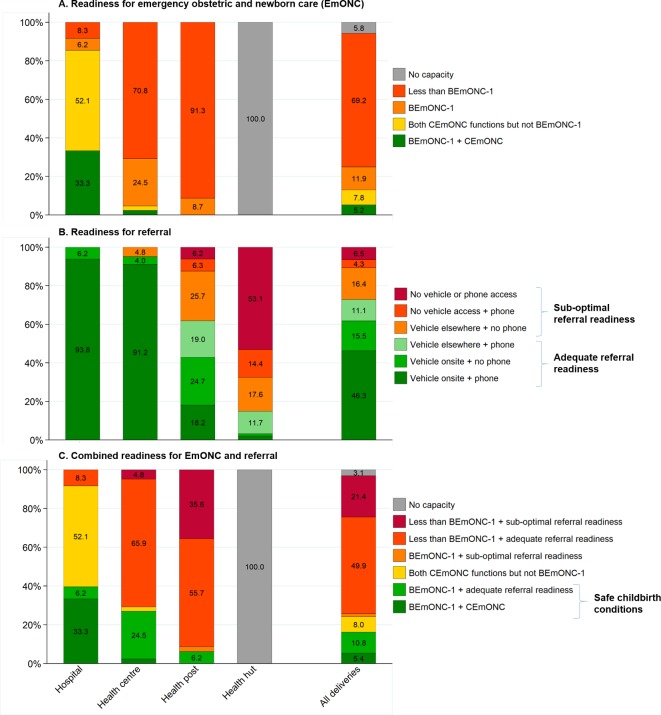
Results: Births in facilities increased from 47% in 1992 to 80% in 2016, driven by births in lower-level health posts, where half of facility births now occur. Caesarean rates in rural areas more than doubled but only to 3.7%, indicating minor improvements in EmONC access. Only 9% of health posts had full readiness for basic EmONC, and 62% had adequate referral readiness (vehicle on-site or telephone and vehicle access elsewhere). Although public facilities accounted for three-quarters of all births in 2016, only 16% of such births occurred in facilities able to provide adequate combined readiness for EmONC and referral.
Conclusions: Our findings imply that many lower-level public facilities-the most common place of birth in Senegal-are unable to treat or refer women with obstetric complications, especially in rural areas. In light of rising lower-level facility births in Senegal and elsewhere, improvements in EmONC and referral readiness are urgently needed to accelerate reductions in maternal and perinatal mortality.
Keywords: Senegal; emergency obstetric care; maternal health; readiness; referral.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Readiness of health facilities to provide safe childbirth in Liberia: a cross-sectional analysis of population surveys, facility censuses and facility birth records.BMC Pregnancy Childbirth. 2022 Dec 20;22(1):952. doi: 10.1186/s12884-022-05301-x. BMC Pregnancy Childbirth. 2022. PMID: 36539750 Free PMC article.
-
Emergency obstetric and neonatal care availability, use, and quality: a cross-sectional study in the city of Lubumbashi, Democratic Republic of the Congo, 2011.BMC Pregnancy Childbirth. 2017 Jan 19;17(1):40. doi: 10.1186/s12884-017-1224-9. BMC Pregnancy Childbirth. 2017. PMID: 28103822 Free PMC article.
-
Referral patterns through the lens of health facility readiness to manage obstetric complications: national facility-based results from Ghana.Reprod Health. 2019 Feb 18;16(1):19. doi: 10.1186/s12978-019-0684-y. Reprod Health. 2019. PMID: 30777082 Free PMC article.
-
Barriers to access and utilization of emergency obstetric care at health facilities in sub-Saharan Africa: a systematic review of literature.Syst Rev. 2018 Nov 13;7(1):183. doi: 10.1186/s13643-018-0842-2. Syst Rev. 2018. PMID: 30424808 Free PMC article.
-
Triangulating data sources for further learning from and about the MDSR in Ethiopia: a cross-sectional review of facility based maternal death data from EmONC assessment and MDSR system.BMC Pregnancy Childbirth. 2020 Apr 9;20(1):206. doi: 10.1186/s12884-020-02899-8. BMC Pregnancy Childbirth. 2020. PMID: 32272930 Free PMC article. Review.
Cited by
-
Beyond proximity: an observational study of stillbirth rates and emergency obstetric and newborn care accessibility in The Gambia.BMJ Glob Health. 2025 Apr 3;10(4):e016579. doi: 10.1136/bmjgh-2024-016579. BMJ Glob Health. 2025. PMID: 40185490 Free PMC article.
-
Does hospital variation in intrapartum-related perinatal mortality among caesarean births reflect differences in quality of care? Cross-sectional study in 21 hospitals in Burkina Faso.BMJ Open. 2022 Oct 6;12(10):e055241. doi: 10.1136/bmjopen-2021-055241. BMJ Open. 2022. PMID: 36202588 Free PMC article. Clinical Trial.
-
Stillbirth maternity care measurement and associated factors in population-based surveys: EN-INDEPTH study.Popul Health Metr. 2021 Feb 8;19(Suppl 1):11. doi: 10.1186/s12963-020-00240-1. Popul Health Metr. 2021. PMID: 33557874 Free PMC article.
-
Mixed vulnerabilities: the biological risk of high parity is aggravated by emergency referral in Benin, Malawi, Tanzania and Uganda.Int J Equity Health. 2025 Jan 20;24(1):19. doi: 10.1186/s12939-025-02379-5. Int J Equity Health. 2025. PMID: 39833887 Free PMC article.
-
Readiness of health facilities to provide safe childbirth in Liberia: a cross-sectional analysis of population surveys, facility censuses and facility birth records.BMC Pregnancy Childbirth. 2022 Dec 20;22(1):952. doi: 10.1186/s12884-022-05301-x. BMC Pregnancy Childbirth. 2022. PMID: 36539750 Free PMC article.
References
-
- UNECA, AU, ADB . MDG report 2015: assessing progress in Africa toward the millennium development goals. Addis Ababa, Ethiopia: United nations economic Commission for Africa, African Union, African development bank and United nations development programme, 2015. Available: http://www.undp.org/content/undp/en/home/librarypage/mdg/mdg-reports/afr... [Accessed Nov 2019].
-
- Alkema L, Chou D, Hogan D, et al. . Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the un maternal mortality estimation Inter-Agency group. Lancet 2016;387:462–74. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- The Inter-agency Group for Child Mortality Estimation (UN IGME), UNICEF, WHO . Levels and trends in child mortality. Report 2015. New York, USA: UNICEF, 2015. Available: https://childmortality.org/files_v20/download/IGME%20Report%202015_9_3%2... [Accessed Nov 2019].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical