

Improving lung cancer diagnosis by combining exhaled-breath data and clinical parameters
- PMID: 32201682
- PMCID: PMC7073409
- DOI: 10.1183/23120541.00221-2019
Improving lung cancer diagnosis by combining exhaled-breath data and clinical parameters
Abstract
Introduction: Exhaled-breath analysis of volatile organic compounds could detect lung cancer earlier, possibly leading to improved outcomes. Combining exhaled-breath data with clinical parameters may improve lung cancer diagnosis.
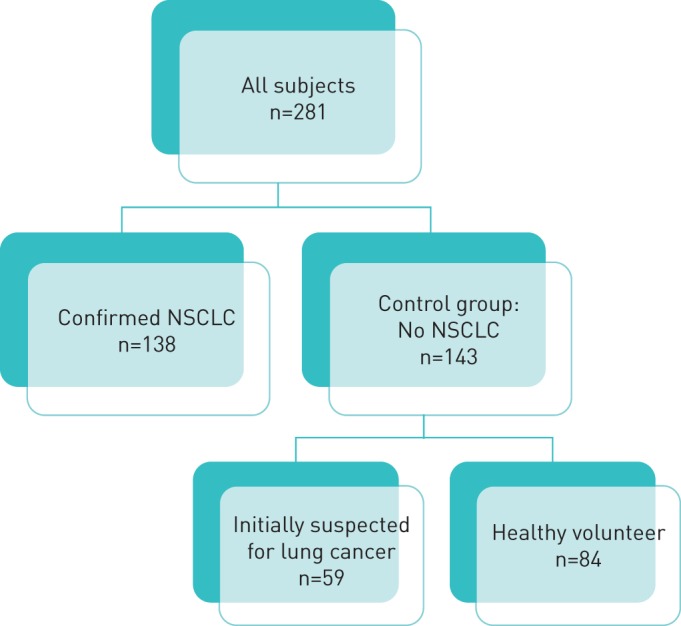
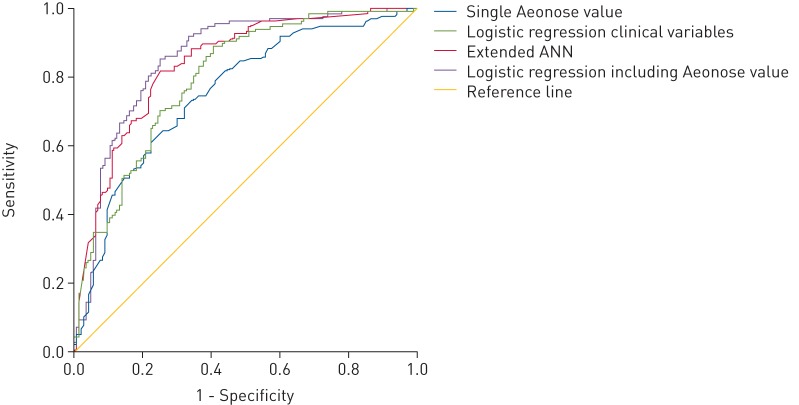
Methods: Based on data from a previous multi-centre study, this article reports additional analyses. 138 subjects with non-small cell lung cancer (NSCLC) and 143 controls without NSCLC breathed into the Aeonose. The diagnostic accuracy, presented as area under the receiver operating characteristic curve (AUC-ROC), of the Aeonose itself was compared with 1) performing a multivariate logistic regression analysis of the distinct clinical parameters obtained, and 2) using this clinical information beforehand in the training process of the artificial neural network (ANN) for the breath analysis.
Results: NSCLC patients (mean±sd age 67.1±9.1 years, 58% male) were compared with controls (62.1±7.0 years, 40.6% male). The AUC-ROC of the classification value of the Aeonose itself was 0.75 (95% CI 0.69-0.81). Adding age, number of pack-years and presence of COPD to this value in a multivariate regression analysis resulted in an improved performance with an AUC-ROC of 0.86 (95% CI 0.81-0.90). Adding these clinical variables beforehand to the ANN for classifying the breath print also led to an improved performance with an AUC-ROC of 0.84 (95% CI 0.79-0.89).
Conclusions: Adding readily available clinical information to the classification value of exhaled-breath analysis with the Aeonose, either post hoc in a multivariate regression analysis or a priori to the ANN, significantly improves the diagnostic accuracy to detect the presence or absence of lung cancer.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: S. Kort reports an unrestricted research grant paid to her institution by The eNose Company, Zutphen, during the conduct of the study. Conflict of interest: M. Brusse-Keizer has nothing to disclose. Conflict of interest: J.W. Gerritsen is an employee of The eNose Company, Zutphen. Conflict of interest: J.H. Schouwink has nothing to disclose. Conflict of interest: E. Citgez has nothing to disclose. Conflict of interest: F.H.C. de Jongh has nothing to disclose. Conflict of interest: J. van der Maten has nothing to disclose. Conflict of interest: S. Samii has nothing to disclose. Conflict of interest: M. van den Bogart has nothing to disclose. Conflict of interest: J. van der Palen has nothing to disclose.
Figures
References
-
- Patz EF Jr, Greco E, Gatsonis C, et al. Lung cancer incidence and mortality in National Lung Screening Trial participants who underwent low-dose CT prevalence screening: a retrospective cohort analysis of a randomised, multicentre, diagnostic screening trial. Lancet Oncol 2016; 17: 590–599. doi: 10.1016/S1470-2045(15)00621-X - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources