

Revision of 'golden hour' for hemodynamically unstable trauma patients: an analysis of nationwide hospital-based registry in Japan
- PMID: 32201736
- PMCID: PMC7066640
- DOI: 10.1136/tsaco-2019-000405
Revision of 'golden hour' for hemodynamically unstable trauma patients: an analysis of nationwide hospital-based registry in Japan
Abstract
Background: The 'golden hour' is a well-known concept, suggesting that shortening time from injury to definitive care is critically important for better outcome of trauma patients. However, there was no established evidence to support it. We aimed to validate the association between time to definitive care and mortality in hemodynamically unstable patients for the current trauma care settings.
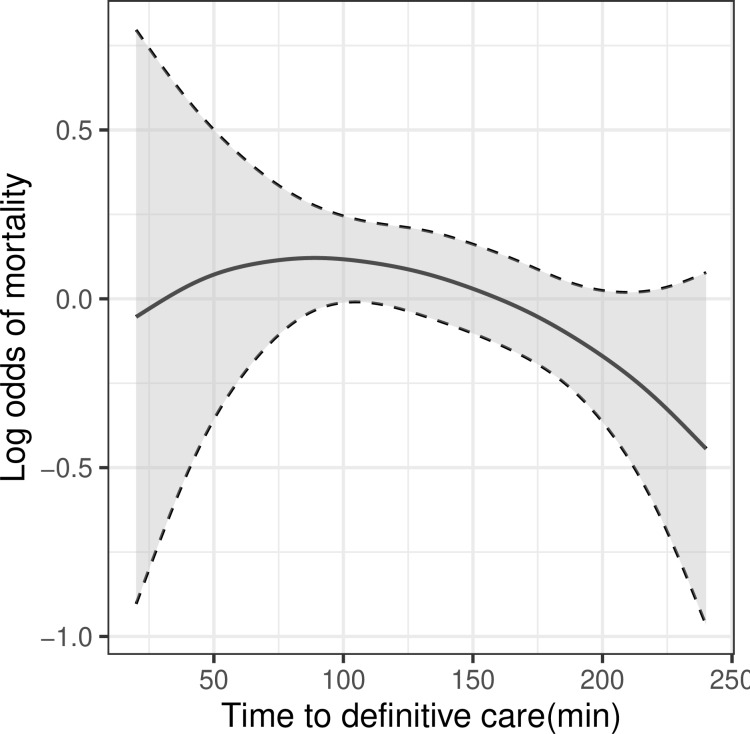
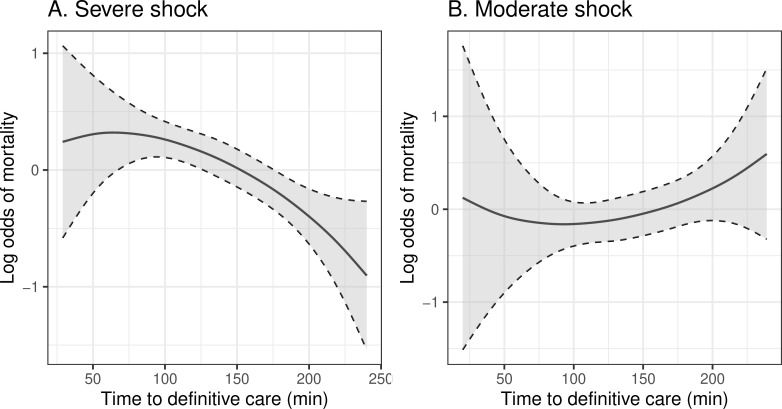
Methods: The data were collected from the Japan Trauma Data Bank between 2006 and 2015. The inclusion criteria were patients with systolic blood pressure (SBP) <90 mm Hg and heart rate (HR) >110 beats/min or SBP <70 mm Hg who underwent definitive care within 4 hours from the onset of injury and survived for more than 4 hours. The outcome measure was in-hospital mortality. We evaluated the relationship between time to definitive care and mortality using the generalized additive model (GAM). Subgroup analysis was also conducted using GAM after dividing the patients into the severe (SBP <70 mm Hg) and moderate (SBP ≥70 mm Hg and <90 mm Hg, and HR >110 beats/min) shock group.
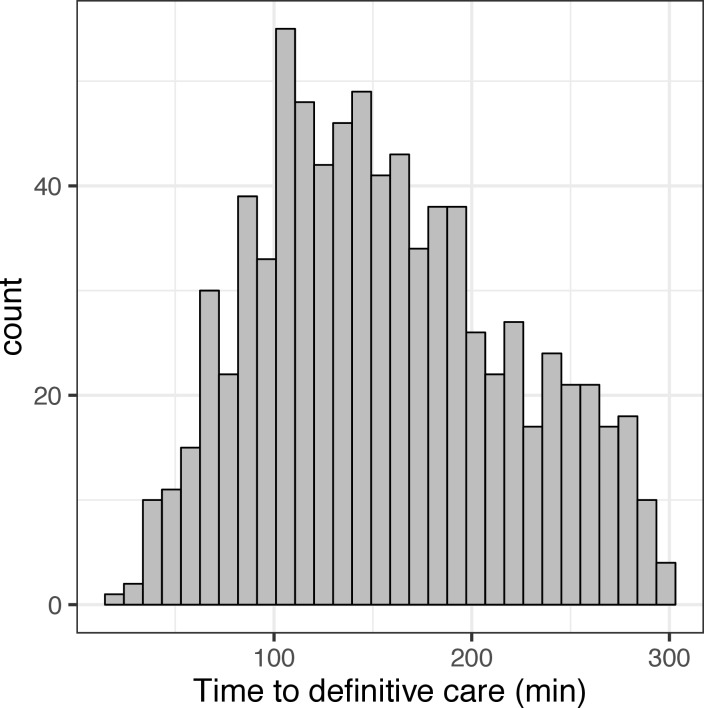
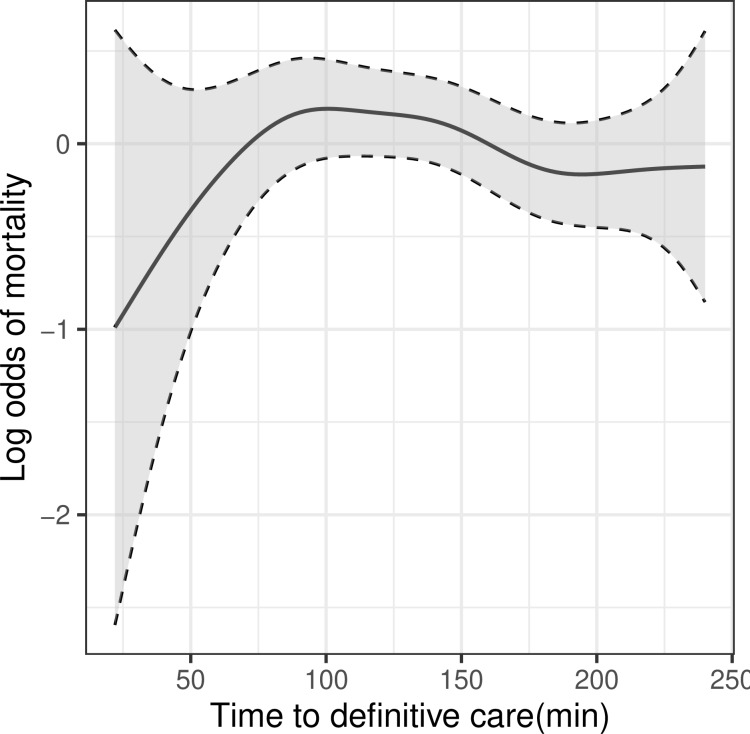
Results: 1169 patients were enrolled in this study. Of these, 386 (33.0%) died. Median time from injury to definitive care was 137 min. Only 61 patients (5.2%) received definitive care within 60 min. The GAM models demonstrated that mortality remained stable for the early phase, followed by a decrease over time. The severe shock group presented with a paradoxical decline of mortality with time, whereas the moderate shock group had a time-dependent increase in mortality.
Discussion: We did not observe the association of shorter time to definitive care with a decrease in mortality. However, this was likely an offset result of severe and moderate shock groups. The result indicated that early definitive care could have a positive impact on survival outcome of patients with moderate shock.
Level of evidence: Level Ⅳ, prognostic study.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Cowley RA. A total emergency medical system for the state of Maryland. Md State Med J 1975;24:37–45. - PubMed
-
- Newgard CD, Meier EN, Bulger EM, Buick J, Sheehan K, Lin S, Minei JP, Barnes-Mackey RA, Brasel K, et al. ROC Investigators . Revisiting the "Golden Hour": An Evaluation of Out-of-Hospital Time in Shock and Traumatic Brain Injury. Ann Emerg Med 2015;66:30–41. 10.1016/j.annemergmed.2014.12.004 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials