

Optimal Level of Femoral Neck for Predicting Postoperative Stem Anteversion in Total Hip Arthroplasty for Crowe Type I Dysplastic Hip
- PMID: 32202054
- PMCID: PMC7189059
- DOI: 10.1111/os.12647
Optimal Level of Femoral Neck for Predicting Postoperative Stem Anteversion in Total Hip Arthroplasty for Crowe Type I Dysplastic Hip
Abstract
Objective: This study aimed to investigate the optimal level of femoral neck for measuring femoral anteversion to predict postoperative stem anteversion in Crowe type I developmental dysplasia of the hip.
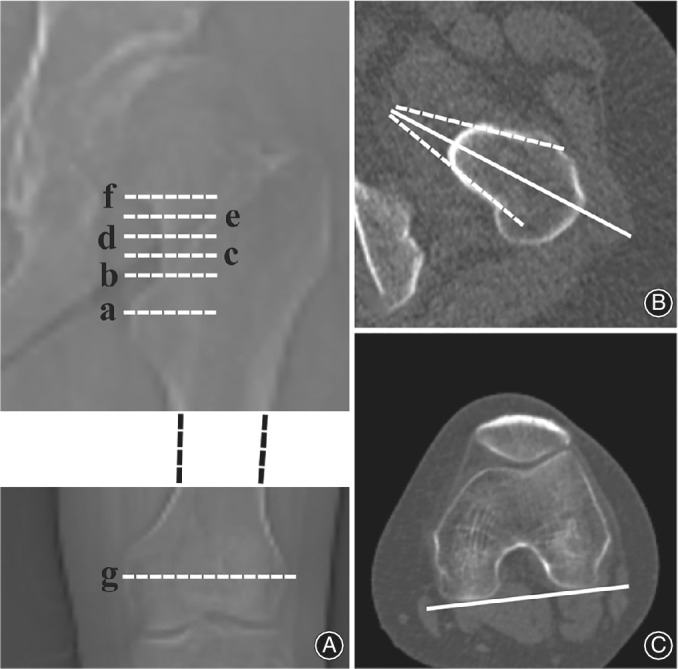
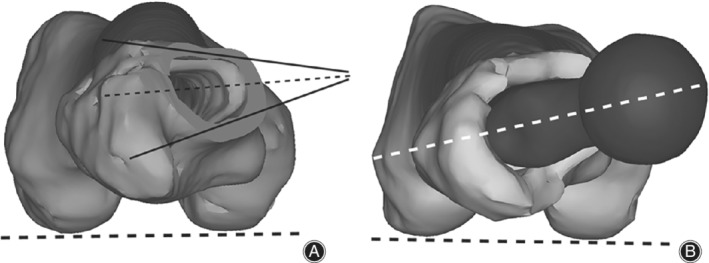
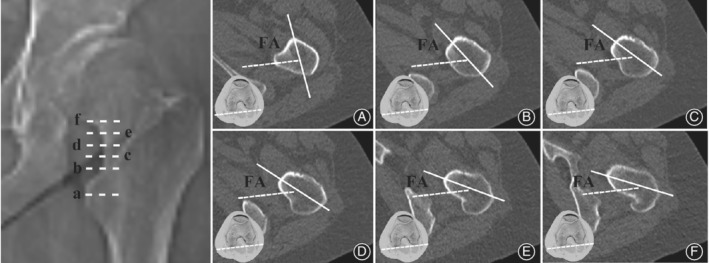
Methods: This retrospective study analyzed 108 Crowe type I hips that underwent THA between January 2016 and December 2017, including 70 women and 19 men with a mean age of 63.08 ± 9.13 (range, 41-83) years. The single-wedge stem was used in 37 hips, the double-wedge stem was used in 71 hips. Computed tomography scans were performed pre- and post-operation. Femoral anteversion at six levels of the proximal femur were measured via preoperative two-dimensional computed tomography. Femoral anteversion at the level of the femoral neck osteotomy plane and postoperative stem anteversion were measured via three-dimensional reconstructed models.
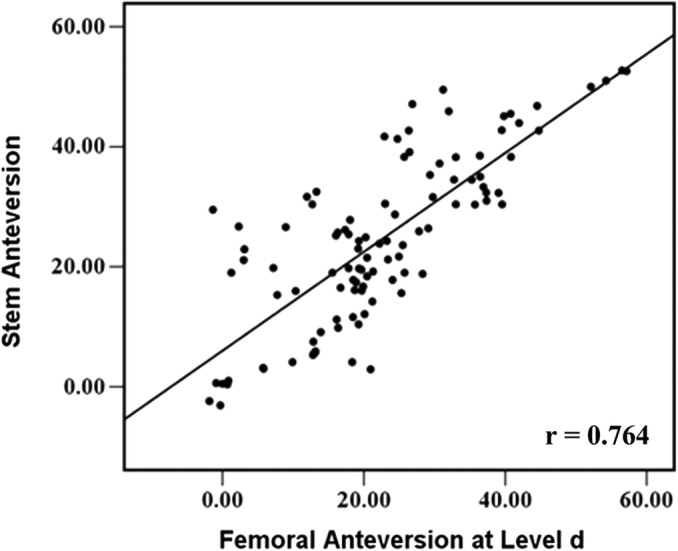
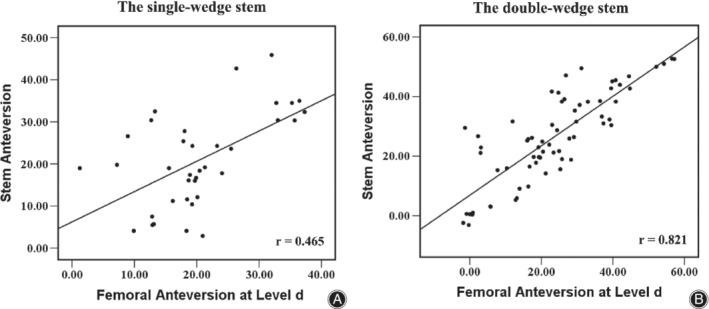
Results: The mean follow-up period was 18.5 months (range, 12-27). The mean preoperative Harris Hip Score was 51.5 ± 8.7 and improved to 90.4 ± 7.8 (P < 0.001) by the last follow-up. There were no intraoperative fractures, and no infections occurred during the follow-up period. Two patients developed deep venous thrombosis. There was no sign of prosthetic loosening in all hips. No significant correlations were found between the height of the femoral neck osteotomy plane and postoperative stem anteversion (r = -0.119, P = 0.220). Femoral anteversion decreased gradually from 64.00° ± 10.51° at the center of lesser trochanter to 15.21° ± 13.31° at the head-neck junction, which was changed from more to less than stem anteversion (24.37° ± 13.86°). The femoral anteversion at femoral head-neck junction (15.21° ± 13.31°) was significantly less than postoperative stem anteversion (P = 0.000), with a difference of -9.16° ± 9.27°. The femoral anteversion at the level of the osteotomy plane (28.48° ± 15.34°) was significantly more than the postoperative stem anteversion (P = 0.000), with a difference of 4.11° ± 9.56°. Among all six levels and the level of osteotomy, femoral anteversion at the 10-mm level above the proximal base of lesser trochanter (22.65 ± 12.92) displayed the smallest difference (-1.72° ± 8.90°) and a good correlation (r = 0.764) with postoperative stem anteversion for all 108 hips, with a moderate correlation of 0.465 for single-wedge stem hips and an excellent correlation of 0.821 for double-wedge stem hips.
Conclusion: For Crowe type I hips, femoral anteversion would be different if it was measured via different levels of the femoral neck. The 10-mm level above the proximal base of the lesser trochanter could be an optimum choice for measuring femoral anteversion to predict postoperative stem anteversion.
Keywords: Developmental dysplasia; Femoral anteversion; Hip; Stem anteversion; Total hip arthroplasty.
© 2020 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures
References
-
- Ferguson RJ, Palmer AJR, Taylor A, Porter ML, Malchau H, Glyn‐Jones S. Hip replacement. Lancet, 2018, 392: 1662–1671. - PubMed
-
- Greber EM, Pelt CE, Gililland JM, Anderson MB, Erickson JA, Peters CL. Challenges in total hip arthroplasty in the setting of developmental dysplasia of the hip. J Arthroplasty, 2017, 32: S38–S44. - PubMed
-
- Li H, Wang Y, Oni JK, et al The role of femoral neck anteversion in the development of osteoarthritis in dysplastic hips. Bone Joint J, 2014, 96‐b: 1586–1593. - PubMed
-
- Sugano N, Noble PC, Kamaric E, Salama JK, Ochi T, Tullos HS. The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br, 1998, 80: 711–719. - PubMed
-
- Noble PC, Kamaric E, Sugano N, et al Three‐dimensional shape of the dysplastic femur: implications for THR. Clin Orthop Relat Res, 2003, 417: 27–40. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
