

Osteosarcopenia: epidemiology, diagnosis, and treatment-facts and numbers
- PMID: 32202056
- PMCID: PMC7296259
- DOI: 10.1002/jcsm.12567
Osteosarcopenia: epidemiology, diagnosis, and treatment-facts and numbers
Abstract
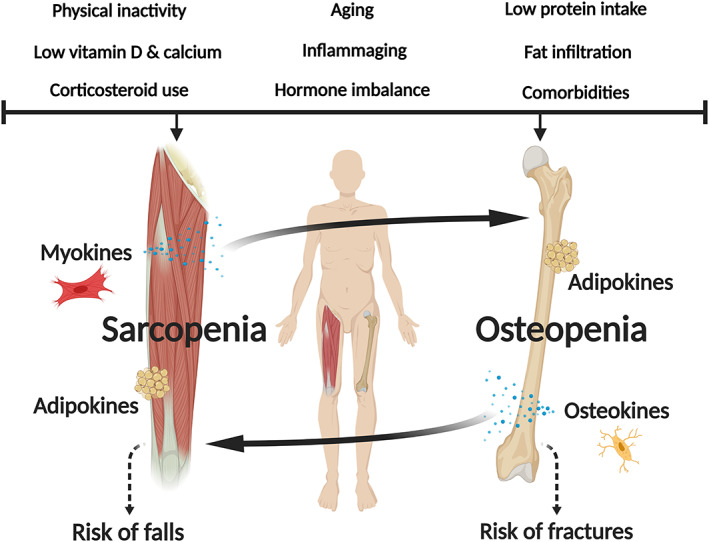
Background: Osteosarcopenia, the presence of osteopenia/osteoporosis and sarcopenia, is an emerging geriatric giant, which poses a serious global health burden.
Methods and results: The prevalence of osteosarcopenia ranges in community-dwelling older adults [5-37% (≥65 years)] with the highest rates observed in those with fractures (low-trauma fracture: ~46%; hip fracture: 17.1-96.3%). Among 2353 community-dwelling adults, risk factors associated with osteosarcopenia include older age [men: 14.3% (60-64 years) to 59.4% (≥75 years); women: 20.3% (60-64 years) to 48.3% (≥75 years), P < 0.05], physical inactivity [inverse relationship: 0.64, 95% confidence interval (CI) 0.46-0.88 (sexes combined)], low body mass index (inverse relationship: men: 0.84, 95% CI 0.81-0.88; women: 0.77, 95% CI 0.74-0.80), and higher fat mass (men: 1.46, 95% CI 1.11-1.92; women: 2.25, 95% CI 1.71-2.95). Among 148 geriatric inpatients, osteosarcopenic individuals demonstrate poorer nutritional status (mini-nutritional assessment scores: 8.50 ± 2.52 points, P < 0.001) vs. osteoporosis or sarcopenia alone, while among 253 older Australians, osteosarcopenia is associated with impaired balance and functional capacity [odds ratios (ORs): 2.56-7.19; P < 0.05] vs. non-osteosarcopenia. Osteosarcopenia also associates with falls (ORs: 2.83-3.63; P < 0.05), fractures (ORs: 3.86-4.38; P < 0.05), and earlier death [hazard ratio (1-year follow-up): 1.84, 95% CI; 0.69-4.92, P = 0.023] vs. non-osteosarcopenia.
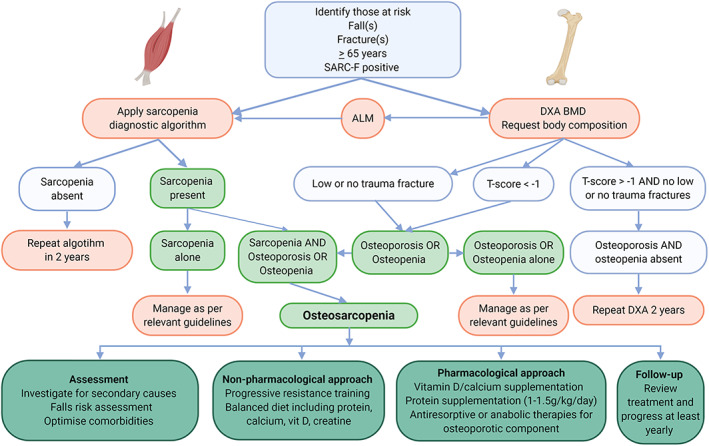
Conclusions: This syndrome is expected to grow in age-related and disease-related states, a likely consequence of immunosenescence coinciding with increased sedentarism, obesity, and fat infiltration of muscle and bone. Evidence suggests the pathophysiology of osteosarcopenia includes genetic polymorphisms, reduced mechanical loading, and impaired endocrine functioning, as well as altered crosstalk between muscle, bone, and fat cells. Clinicians should screen for osteosarcopenia via imaging methods (i.e. dual-energy X-ray absorptiometry) to quantify muscle and bone mass, in addition to assessing muscle strength (i.e. grip strength) and functional capacity (i.e. gait speed). A comprehensive geriatric assessment, including medical history and risk factors, must also be undertaken. Treatment of this syndrome should include osteoporotic drugs [bone anabolics/antiresorptives (i.e. teriparatide, denosumab, bisphosphates)] where indicated, and progressive resistance and balance exercises (at least 2-3 times/week). To maximize musculoskeletal health, nutritional recommendations [protein (1.2-1.5 g/kg/day), vitamin D (800-1000 IU/day), calcium (1300 mg/day), and creatine (3-5 g/day)] must also be met. It is anticipated that diagnosis and treatment for osteosarcopenia will become part of routine healthcare in the future. However, further work is required to identify biomarkers, which, in turn, may increase diagnosis, risk stratification, and targeted treatments to improve health outcomes.
Keywords: Bone; Falls; Fractures; Mortality; Muscle; Osteosarcopenia.
© 2020 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors have no conflict of interest regarding this work.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
