

Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer's disease in patients with rheumatoid arthritis and psoriasis
- PMID: 32203525
- PMCID: PMC7089534
- DOI: 10.1371/journal.pone.0229819
Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer's disease in patients with rheumatoid arthritis and psoriasis
Abstract
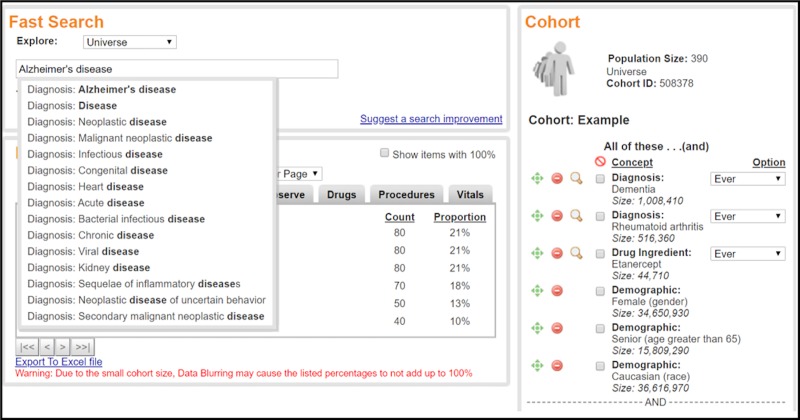
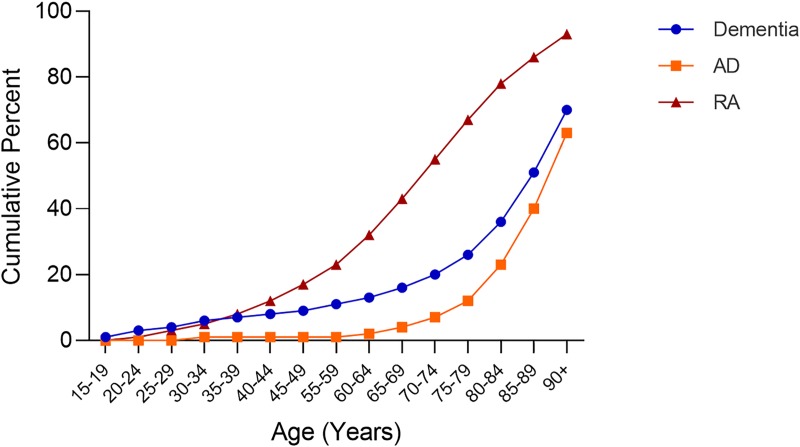
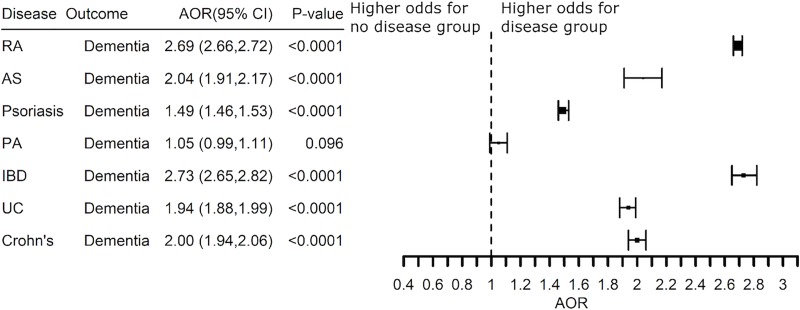
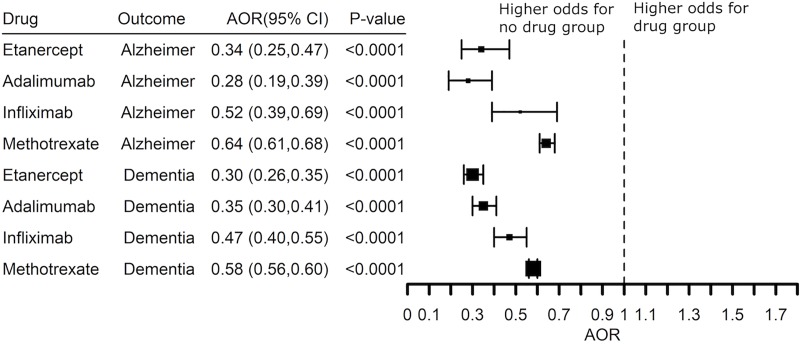
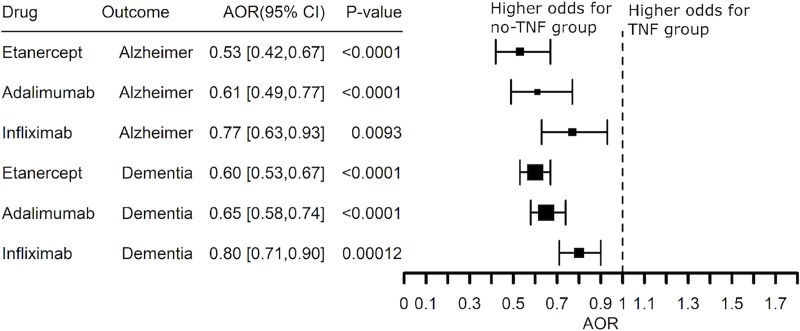
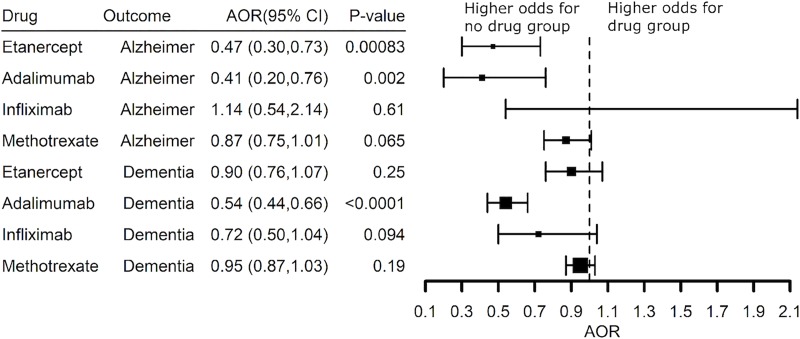
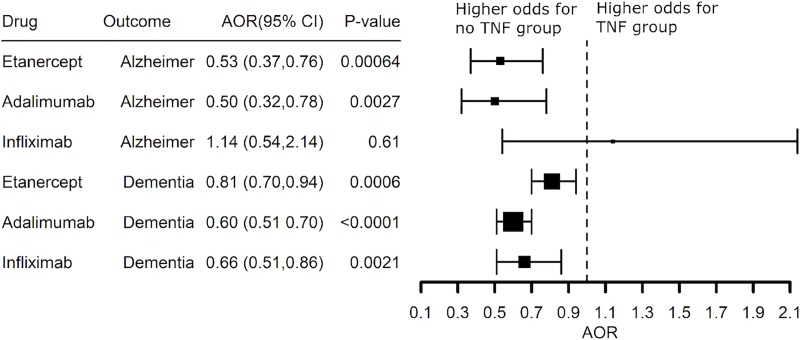
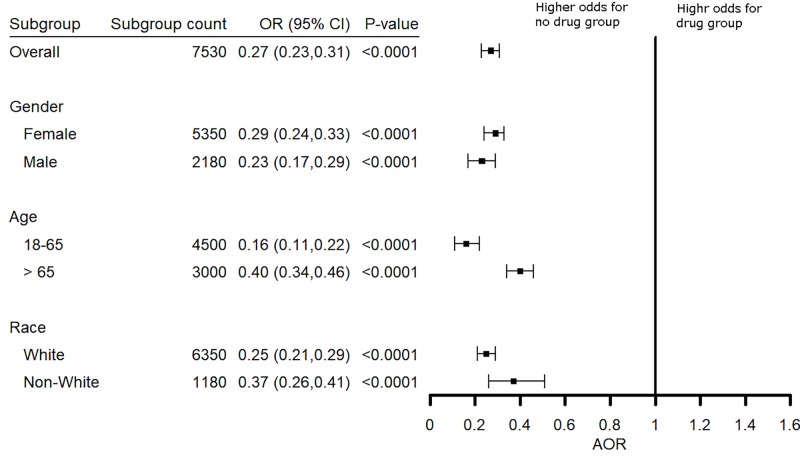
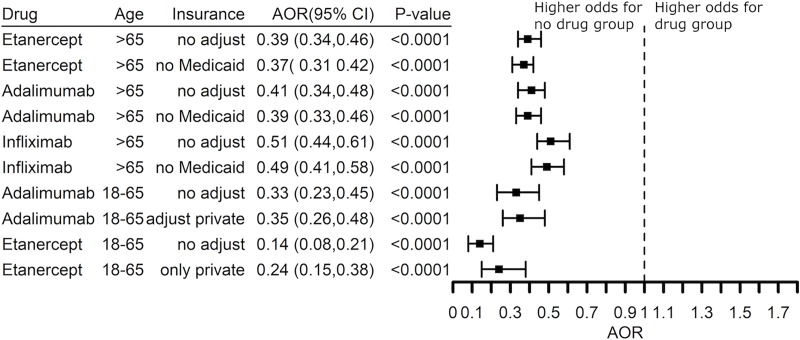
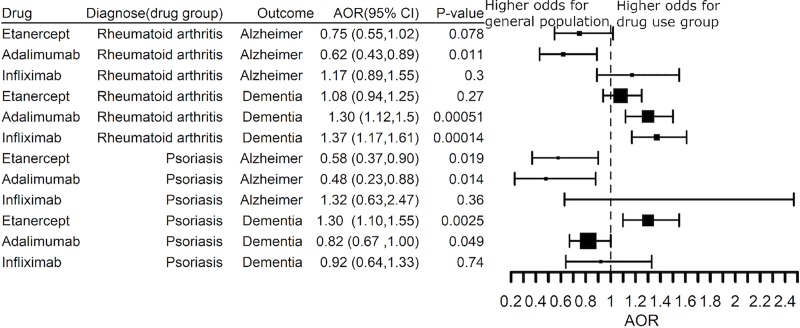
This large, retrospective case-control study of electronic health records from 56 million unique adult patients examined whether or not treatment with a Tumor Necrosis Factor (TNF) blocking agent is associated with lower risk for Alzheimer's disease (AD) in patients with rheumatoid arthritis (RA), psoriasis, and other inflammatory diseases which are mediated in part by TNF and for which a TNF blocker is an approved treatment. The analysis compared the diagnosis of AD as an outcome measure in patients receiving at least one prescription for a TNF blocking agent (etanercept, adalimumab, and infliximab) or for methotrexate. Adjusted odds ratios (AORs) were estimated using the Cochran-Mantel-Haenszel (CMH) method and presented with 95% confidence intervals (CIs) and p-values. RA was associated with a higher risk for AD (Adjusted Odds Ratio (AOR) = 2.06, 95% Confidence Interval: (2.02-2.10), P-value <0.0001) as did psoriasis (AOR = 1.37 (1.31-1.42), P <0.0001), ankylosing spondylitis (AOR = 1.57 (1.39-1.77), P <0.0001), inflammatory bowel disease (AOR = 2.46 (2.33-2.59), P < 0.0001), ulcerative colitis (AOR = 1.82 (1.74-1.91), P <0.0001), and Crohn's disease (AOR = 2.33 (2.22-2.43), P <0.0001). The risk for AD in patients with RA was lower among patients treated with etanercept (AOR = 0.34 (0.25-0.47), P <0.0001), adalimumab (AOR = 0.28 (0.19-0.39), P < 0.0001), or infliximab (AOR = 0.52 (0.39-0.69), P <0.0001). Methotrexate was also associated with a lower risk for AD (AOR = 0.64 (0.61-0.68), P <0.0001), while lower risk was found in patients with a prescription history for both a TNF blocker and methotrexate. Etanercept and adalimumab also were associated with lower risk for AD in patients with psoriasis: AOR = 0.47 (0.30-0.73 and 0.41 (0.20-0.76), respectively. There was no effect of gender or race, while younger patients showed greater benefit from a TNF blocker than did older patients. This study identifies a subset of patients in whom systemic inflammation contributes to risk for AD through a pathological mechanism involving TNF and who therefore may benefit from treatment with a TNF blocking agent.
Conflict of interest statement
M.E.G is an employee of Tetra Therapeutics. This commercial affiliation does not alter the adherence of M.E.G to PLOS ONE policies on sharing data and materials.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
