

Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis
- PMID: 32203549
- PMCID: PMC7089422
- DOI: 10.1371/journal.pmed.1003062
Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis
Abstract
Background: Circulating lipoprotein lipids cause coronary heart disease (CHD). However, the precise way in which one or more lipoprotein lipid-related entities account for this relationship remains unclear. Using genetic instruments for lipoprotein lipid traits implemented through multivariable Mendelian randomisation (MR), we sought to compare their causal roles in the aetiology of CHD.
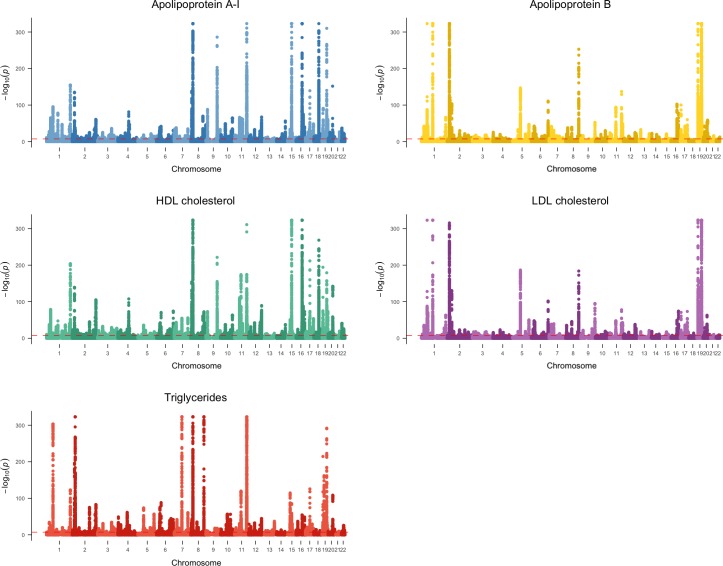
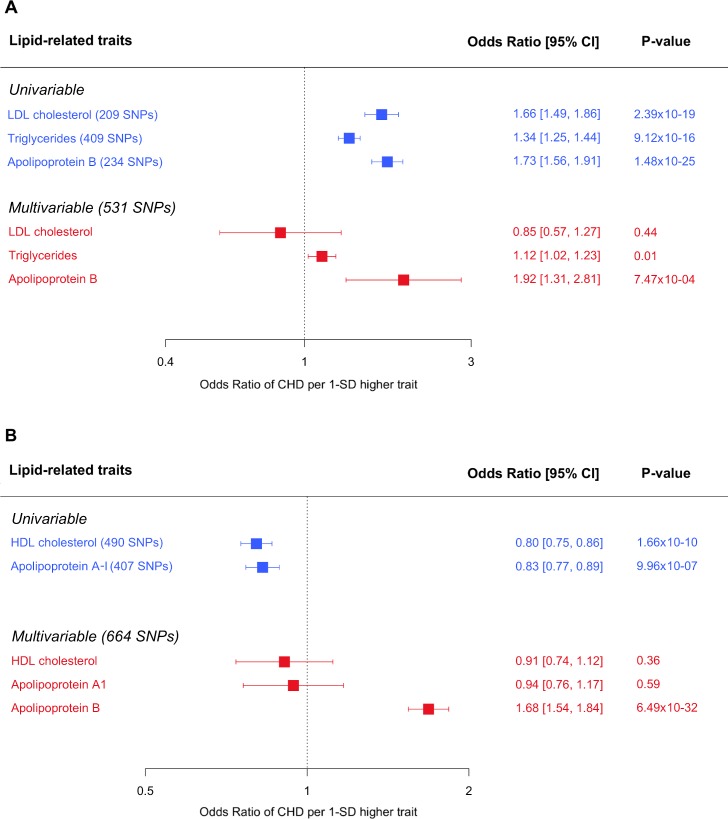
Methods and findings: We conducted a genome-wide association study (GWAS) of circulating non-fasted lipoprotein lipid traits in the UK Biobank (UKBB) for low-density lipoprotein (LDL) cholesterol, triglycerides, and apolipoprotein B to identify lipid-associated single nucleotide polymorphisms (SNPs). Using data from CARDIoGRAMplusC4D for CHD (consisting of 60,801 cases and 123,504 controls), we performed univariable and multivariable MR analyses. Similar GWAS and MR analyses were conducted for high-density lipoprotein (HDL) cholesterol and apolipoprotein A-I. The GWAS of lipids and apolipoproteins in the UKBB included between 393,193 and 441,016 individuals in whom the mean age was 56.9 y (range 39-73 y) and of whom 54.2% were women. The mean (standard deviation) lipid concentrations were LDL cholesterol 3.57 (0.87) mmol/L and HDL cholesterol 1.45 (0.38) mmol/L, and the median triglycerides was 1.50 (IQR = 1.11) mmol/L. The mean (standard deviation) values for apolipoproteins B and A-I were 1.03 (0.24) g/L and 1.54 (0.27) g/L, respectively. The GWAS identified multiple independent SNPs associated at P < 5 × 10-8 for LDL cholesterol (220), apolipoprotein B (n = 255), triglycerides (440), HDL cholesterol (534), and apolipoprotein A-I (440). Between 56%-93% of SNPs identified for each lipid trait had not been previously reported in large-scale GWASs. Almost half (46%) of these SNPs were associated at P < 5 × 10-8 with more than one lipid-related trait. Assessed individually using MR, LDL cholesterol (odds ratio [OR] 1.66 per 1-standard-deviation-higher trait; 95% CI: 1.49-1.86; P < 0.001), triglycerides (OR 1.34; 95% CI: 1.25-1.44; P < 0.001) and apolipoprotein B (OR 1.73; 95% CI: 1.56-1.91; P < 0.001) had effect estimates consistent with a higher risk of CHD. In multivariable MR, only apolipoprotein B (OR 1.92; 95% CI: 1.31-2.81; P < 0.001) retained a robust effect, with the estimate for LDL cholesterol (OR 0.85; 95% CI: 0.57-1.27; P = 0.44) reversing and that of triglycerides (OR 1.12; 95% CI: 1.02-1.23; P = 0.01) becoming weaker. Individual MR analyses showed a 1-standard-deviation-higher HDL cholesterol (OR 0.80; 95% CI: 0.75-0.86; P < 0.001) and apolipoprotein A-I (OR 0.83; 95% CI: 0.77-0.89; P < 0.001) to lower the risk of CHD, but these effect estimates attenuated substantially to the null on accounting for apolipoprotein B. A limitation is that, owing to the nature of lipoprotein metabolism, measures related to the composition of lipoprotein particles are highly correlated, creating a challenge in making exclusive interpretations on causation of individual components.
Conclusions: These findings suggest that apolipoprotein B is the predominant trait that accounts for the aetiological relationship of lipoprotein lipids with risk of CHD.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: BAF reports receiving grants from Amgen, Merck & Co., Novartis, and Esperion Therapeutics; consulting or advisory board fees from Amgen, Regeneron, Sanofi, Merck & Co., Pfizer, CiVi BioPhama, and KrKA Pharmaceuticals; and grants from Merck & Co., Amgen, Novartis, Novo Nordisk, Regeneron, Sanofi, Pfizer, Eli Lilly, Mylan, Ionis, dalCOR, Silence Therapeutics, Integral Therapeutics, CiVi Pharma, KrKa Phamaceuticals, American College of Cardiology, European Atherosclerosis Society, and European Society of Cardiology. MVH has collaborated with Boehringer Ingelheim in research, and in accordance with the policy of the The Clinical Trial Service Unit and Epidemiological Studies Unit (University of Oxford), did not accept any personal payment. GDS is an Academic Editor on PLOS Medicine's editorial board. All other authors report no potential conflicts of interest.
Figures

References
-
- Cholesterol Treatment Trialist's Collaborators, Fulcher J, O'Connell R, Voysey M, Emberson J, Blackwell L, et al. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. 2015;385(9976):1397–405. 10.1016/S0140-6736(14)61368-4 . - DOI - PubMed
-
- Cholesterol Treatment Trialists' Collaborators, Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670–81. 10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
-
- Cholesterol Treatment Trialists' Collaborators, Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581–90. 10.1016/S0140-6736(12)60367-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
