

A Role for Endoplasmic Reticulum Stress in Intracerebral Hemorrhage
- PMID: 32204394
- PMCID: PMC7140640
- DOI: 10.3390/cells9030750
A Role for Endoplasmic Reticulum Stress in Intracerebral Hemorrhage
Abstract
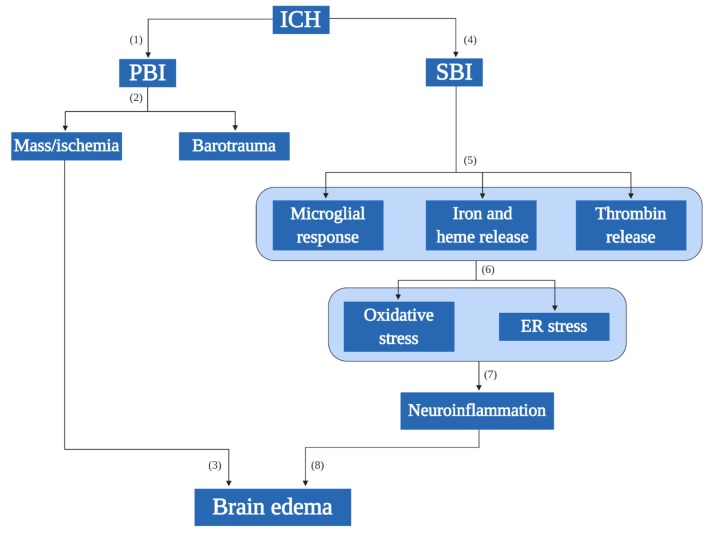
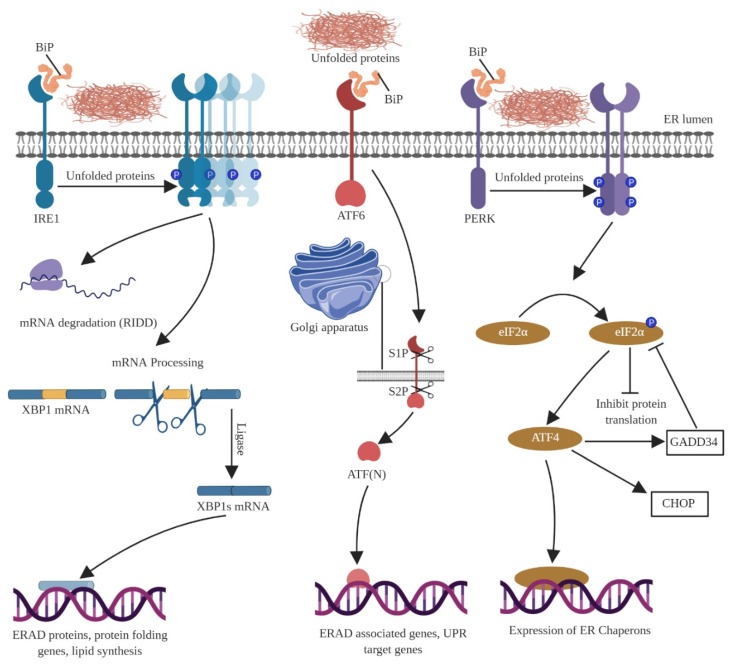
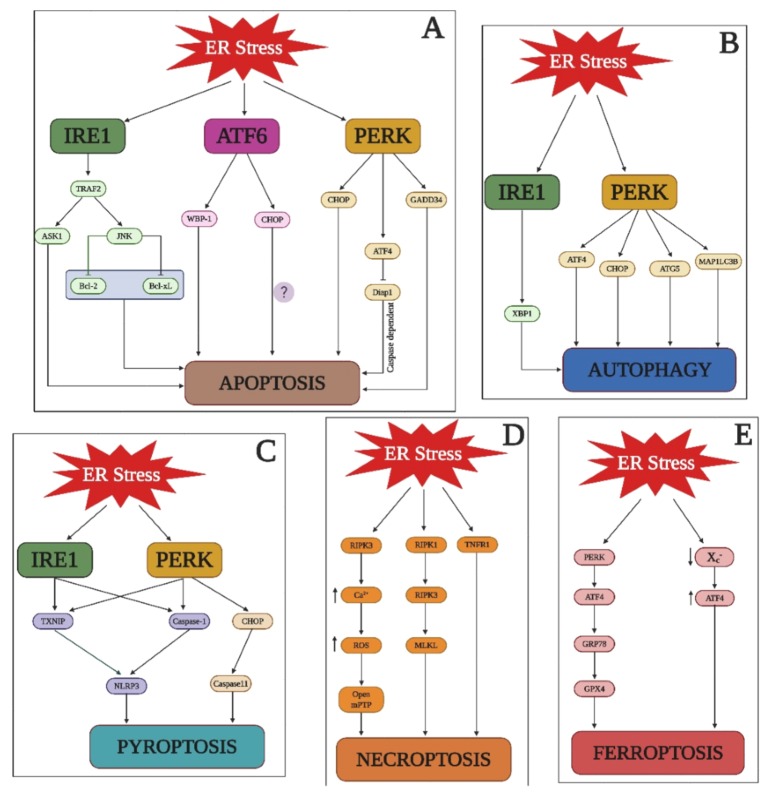
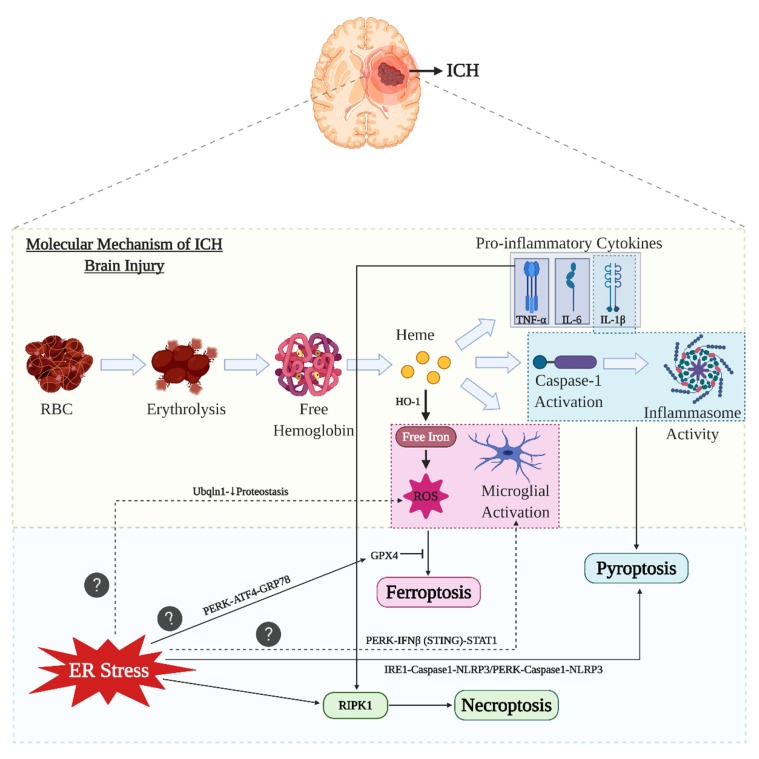
The endoplasmic reticulum (ER) is an intracellular organelle that performs multiple functions, such as lipid biosynthesis, protein folding, and maintaining intracellular calcium homeostasis. Thus, conditions wherein the ER is unable to fold proteins is defined as ER stress, and an inbuilt quality control mechanism, called the unfolded protein response (UPR), is activated during ER stress, which serves as a recovery system that inhibits protein synthesis. Further, based on the severity of ER stress, the response could involve both proapoptotic and antiapoptotic phases. Intracerebral hemorrhage (ICH) is the second most common subtype of cerebral stroke and many lines of evidence have suggested a role for the ER in major neurological disorders. The injury mechanism during ICH includes hematoma formation, which in turn leads to inflammation, elevated intracranial pressure, and edema. A proper understanding of the injury mechanism(s) is required to effectively treat ICH and closing the gap between our current understanding of ER stress mechanisms and ICH injury can lead to valuable advances in the clinical management of ICH.
Keywords: ER stress; ferroptosis; intracerebral hemorrhage; necroptosis; neuroinflammation; pyroptosis; unfolded protein response.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
