

Review
doi: 10.1186/s13054-020-2776-z.
Physiology of the Respiratory Drive in ICU Patients: Implications for Diagnosis and Treatment
Affiliations
- PMID: 32204710
- PMCID: PMC7092542
- DOI: 10.1186/s13054-020-2776-z
Item in Clipboard
Review
Physiology of the Respiratory Drive in ICU Patients: Implications for Diagnosis and Treatment
Crit Care.
.
Erratum in
-
Correction : Selected articles from the annual update in intensive care and emergency medicine 2020.Crit Care. 2024 Mar 21;28(1):94. doi: 10.1186/s13054-024-04856-9. Crit Care. 2024. PMID: 38515200 Free PMC article. No abstract available.
Abstract
This article is one of ten reviews selected from the Annual Update in Intensive Care and Emergency Medicine 2020. Other selected articles can be found online at https://www.biomedcentral.com/collections/annualupdate2020. Further information about the Annual Update in Intensive Care and Emergency Medicine is available from http://www.springer.com/series/8901.
Conflict of interest statement
LH has received grants from Orion Pharma (Finland) and Liberate Medical (USA) and speakers fee from Getinge (Sweden). AJ has received consulting fee from Liberate Medical (USA). HdV has nothing to declare.
Figures
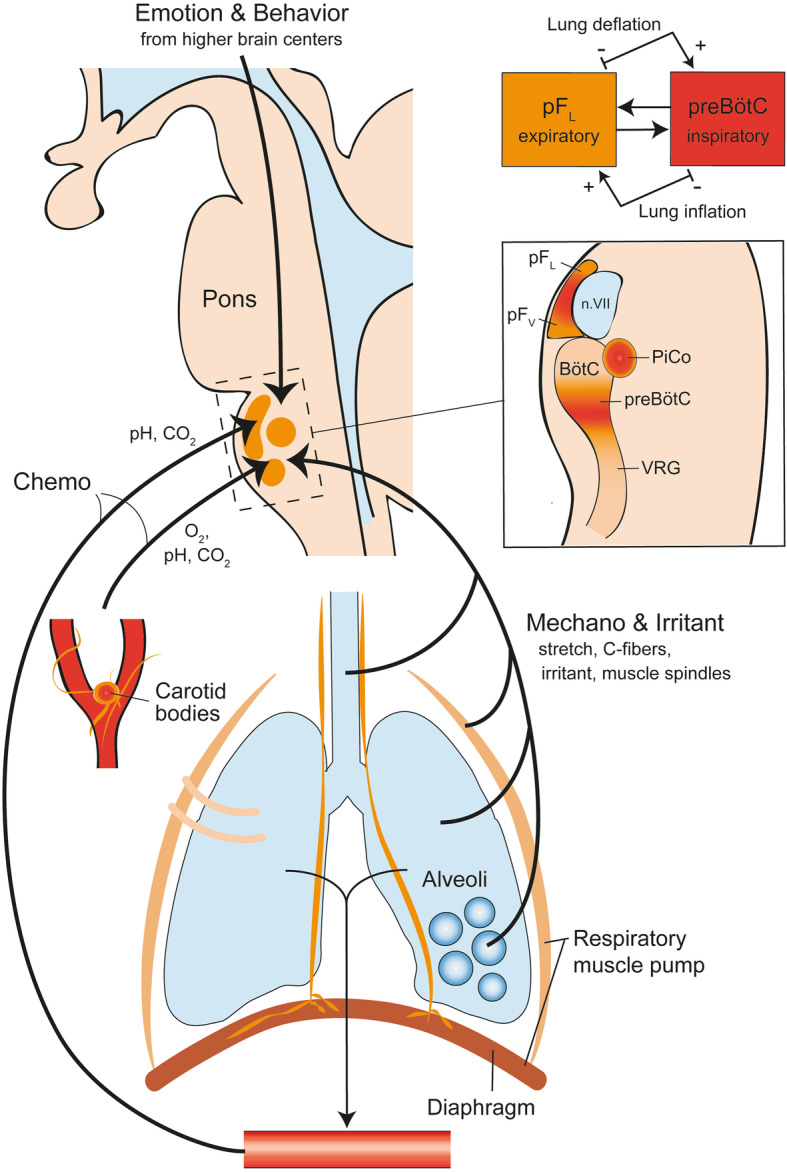
Schematic representation of the anatomy and physiology of respiratory drive. The respiratory centers are located in the medulla and the pons and consist of groups of interneurons that receive information from sources sensitive to chemical, mechanical, behavioral, and emotional stimuli. Important central chemoreceptors are located near the ventral parafacial nucleus (pFV) and are sensitive to direct changes in pH of the cerebrospinal fluid. Peripheral chemoreceptors in the carotid bodies are the primary site sensitive to changes in PaO2, and moderately sensitive to changes in pH and PaCO2. Mechano and irritant receptors are located in the chest wall, airway, lungs, and respiratory muscles. Emotional and behavioral feedback originate in the cerebral cortex and hypothalamus. The pre-Bötzinger complex (preBötC) is the main control center of inspiration, located between the ventral respiratory group (VRG) and the Bötzinger complex (BötC). The post-inspiratory complex (PiCo) is located near the Bötzinger complex. The lateral parafacial nucleus (pFL) controls expiratory activity and has continuous interaction with the pre-Bötzinger complex, to prevent inefficient concomitant activation of inspiratory and expiratory muscle groups: lung inflation depresses inspiratory activity and enhances expiratory activity, which ultimately results in lung deflation. Lung deflation has the opposite effect on these centers
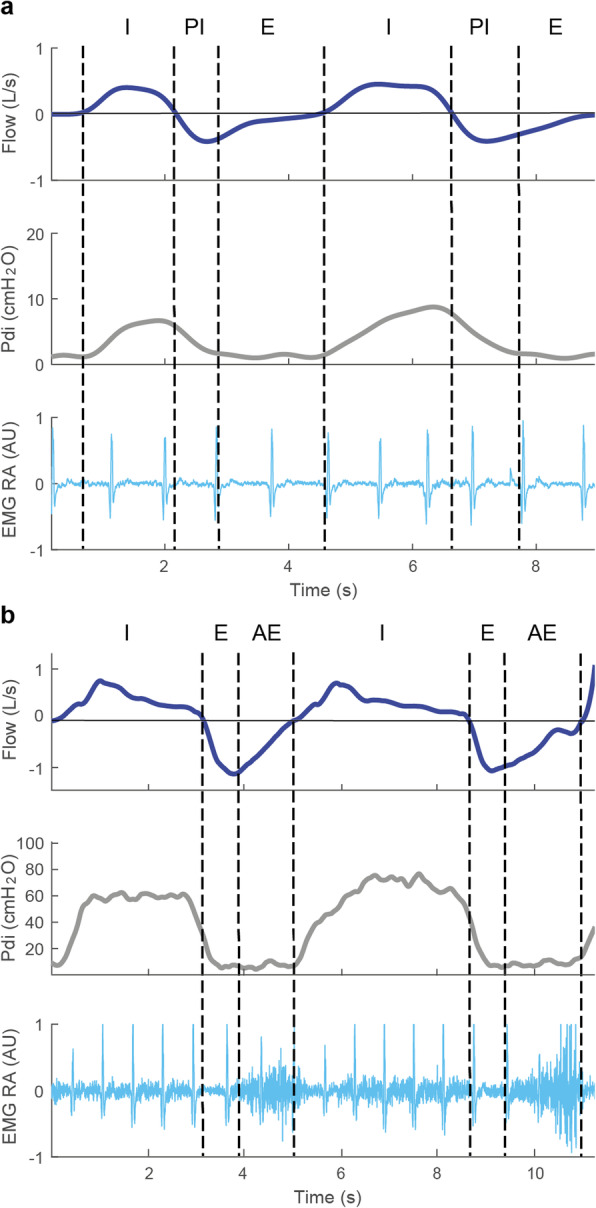
Breathing phases. Flow, transdiaphragmatic pressure (Pdi) and electromyography of the rectus abdominal muscle (EMG RA, in arbitrary units; note that this signal is disturbed with electrocardiogram [EKG] artifacts) during tidal breathing at rest (a) and during high resistive loading (b) in one healthy subject. Vertical dashed lines mark the onset of the different breathing phases. Inspiration (I) is characterized by a steady increase in Pdi and positive flow, and is present during both tidal breathing and high loading. The gradual decrease in Pdi during expiratory flow in (a) is consistent with post-inspiration (PI). Note that the rate of decline in Pdi is much more rapid during high loading. During tidal breathing (a), expiration (E) is characterized by the absence of Pdi and EMG RA activity and occurs after post-inspiration. High loading (b) leads to expiration (AE), which can be recognized by the increase in EMG RA activity. Also, expiration directly follows the inspiratory phase
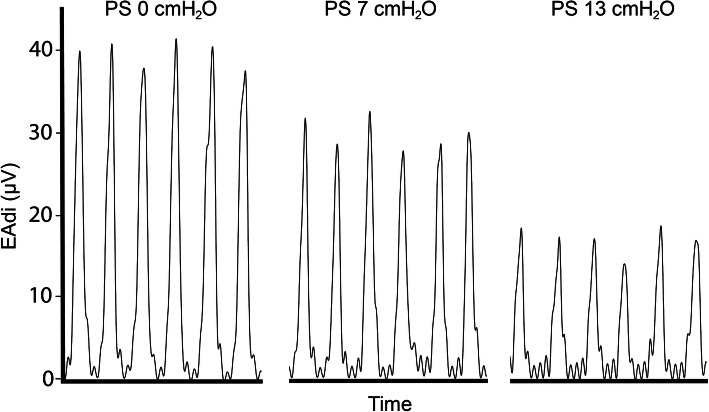
Influence of inspiratory support levels on electrical activity of the diaphragm. Example of a representative patient showing a decrease in electrical activity of the diaphragm (EAdi, in micro volts) in response to increasing levels of inspiratory pressure support (PS)
References
-
- Vaporidi K, Akoumianaka E, Telias I, Goligher EC, Brochard L, Georgopoulos D. Respiratory drive in critically ill patients: pathophysiology and clinical implications. Am J Respir Crit Care Med. 2019. 10.1164/rccm.201903-0596SO. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
