

Non-contact infrared versus axillary and tympanic thermometers in children attending primary care: a mixed-methods study of accuracy and acceptability
- PMID: 32205332
- PMCID: PMC7098492
- DOI: 10.3399/bjgp20X708845
Non-contact infrared versus axillary and tympanic thermometers in children attending primary care: a mixed-methods study of accuracy and acceptability
Erratum in
-
Correction.Br J Gen Pract. 2020 Oct 1;70(699):486. doi: 10.3399/bjgp20X712769. Print 2020 Oct. Br J Gen Pract. 2020. PMID: 33004364 Free PMC article. No abstract available.
Abstract
Background: Guidelines recommend measuring temperature in children presenting with fever using electronic axillary or tympanic thermometers. Non-contact thermometry offers advantages, yet has not been tested against recommended methods in primary care.
Aim: To compare two different non-contact infrared thermometers (NCITs) to axillary and tympanic thermometers in children aged ≤5 years visiting their GP with an acute illness.
Design and setting: Method comparison study with nested qualitative component.
Method: Temperature measurements were taken with electronic axillary (Welch Allyn SureTemp®), electronic tympanic (Braun Thermoscan®), NCIT Thermofocus® 0800, and NCIT Firhealth Forehead. Parents rated acceptability and discomfort. Qualitative interviews explored parents' experiences of the thermometers.
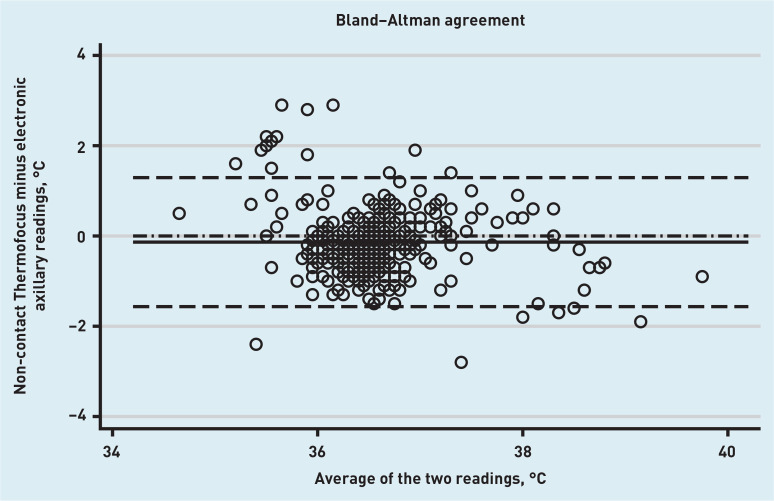
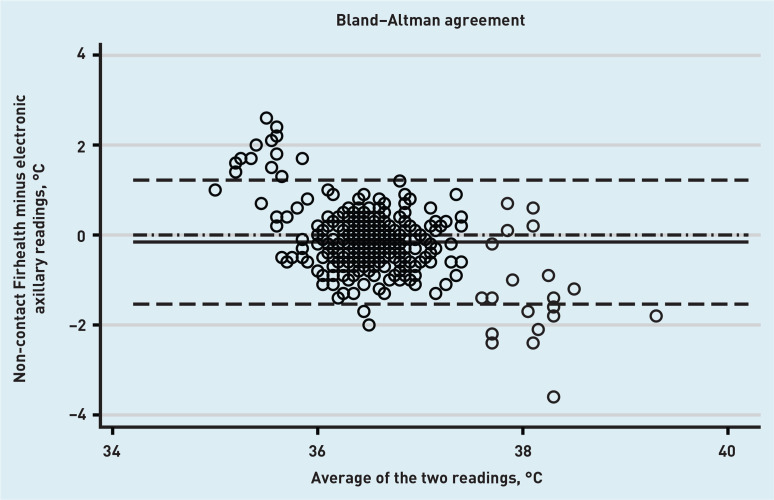
Results: In total, 401 children were recruited (median age 1.6 years, 50.62% male). Mean difference between the Thermofocus NCIT and axillary thermometer was -0.14°C (95% confidence interval [CI] = -0.21 to -0.06°C); lower limit of agreement was -1.57°C (95% CI = -1.69 to -1.44°C) and upper limit 1.29°C (95% CI = 1.16 to 1.42°C). A second NCIT (Firhealth) had similar levels of agreement; however, the limits of agreement between tympanic and axillary thermometers were also wide. Parents expressed a preference for the practicality and comfort of NCITs, and were mostly negative about their child's experience of axillary thermometers. But there was willingness to adopt whichever device was medically recommended.
Conclusion: In a primary care paediatric population, temperature measurements with NCITs varied by >1°C compared with axillary and tympanic approaches. But there was also poor agreement between tympanic and axillary thermometers. Since clinical guidelines often rely on specific fever thresholds, clinicians should interpret peripheral thermometer readings with caution and in the context of a holistic assessment of the child.
Keywords: acute disease; child; fever; primary health care; thermometers.
© British Journal of General Practice 2020.
Figures
References
-
- Hay AD, Heron J, Ness A. The prevalence of symptoms and consultations in pre-school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): a prospective cohort study. Fam Pract. 2005;22(4):367–374. - PubMed
-
- Fleming DM, Smith GE, Charlton JR, et al. Impact of infections on primary care — greater than expected. Commun Dis Public Health. 2002;5(1):7–12. - PubMed
-
- National Institute for Health and Clinical Excellence . Fever in under 5s: assessment and initial management NG143. London: NICE; 2019. https://www.nice.org.uk/guidance/NG143 (accessed 3 Mar 2020). - PubMed
-
- NHS How to take your baby’s temperature: your pregnancy and baby guide. 2020 https://www.nhs.uk/conditions/pregnancy-and-baby/how-to-take-your-babys-... (accessed 3 Mar 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical