

Systematic Review and Meta: Analysis of Aortic Graft Infections following Abdominal Aortic Aneurysm Repair
- PMID: 32206352
- PMCID: PMC7013324
- DOI: 10.1155/2020/9574734
Systematic Review and Meta: Analysis of Aortic Graft Infections following Abdominal Aortic Aneurysm Repair
Abstract
Introduction. Aortic graft infection (AGI) is a rare complication following AAA repair and is associated with high morbidity and mortality. Management is variable, and there are no evidence-based guidelines. The aim of this study was to systematically review and analyse management options for AGI.
Methods: Data was collected between July and August 2018. A full HDAS search was conducted on the following databases: MEDLINE, EMBASE, CINAHL, and PUBMED. Meta-analysis was conducted using RevMan 5 software.
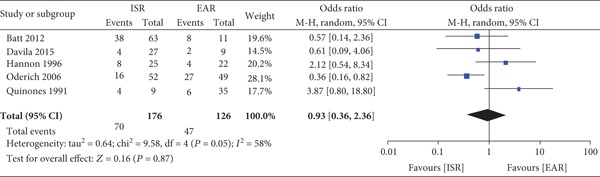
Results: 1,365 patient outcomes were assessed (10 cohort studies and 12 comparative studies). The most common treatment was in situ replacement of the graft (ISR) followed by extra-anatomical replacement (EAR). Various grafts were used for ISR, such as fresh/cryopreserved allograft, venous graft, and prosthetic grafts. No graft material was shown to be superior. Axillobifemoral graft was the commonest type of EAR used. In the majority of cohort studies, ISR was the main treatment for AGI. There was no significant difference in the overall mortality rate (ISR n = 70/176 vs. EAR n = 70/176 vs. EAR P = 0.87). Graft occlusion rate was significantly lower in the ISR group vs. the EAR group (n = 70/176 vs. EAR n = 70/176 vs. EAR P = 0.87). Graft occlusion rate was significantly lower in the ISR group vs. the EAR group (n = 70/176 vs. EAR n = 70/176 vs. EAR P = 0.87). Graft occlusion rate was significantly lower in the ISR group vs. the EAR group (Discussion. In situ replacement is the preferred method of treatment as it had lower rates of occlusion. Further strong evidence is required, such as a multicentre trial to establish a management pathway for the condition.
Copyright © 2020 O. S. Niaz et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Health Quality Improvement Project (HQIP) August 2018, https://www.vsqip.org.uk/reports/2017-annual-report/".
-
- Seeger J. Management of patients with prosthetic vascular graft infection. The American Surgeon. 2000;66(2):166–177. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
