

Acute respiratory distress syndrome-attributable mortality in critically ill patients with sepsis
- PMID: 32206845
- PMCID: PMC7224051
- DOI: 10.1007/s00134-020-06010-9
Acute respiratory distress syndrome-attributable mortality in critically ill patients with sepsis
Abstract
Purpose: Previous studies assessing impact of acute respiratory distress syndrome (ARDS) on mortality have shown conflicting results. We sought to assess the independent association of ARDS with in-hospital mortality among intensive care unit (ICU) patients with sepsis.
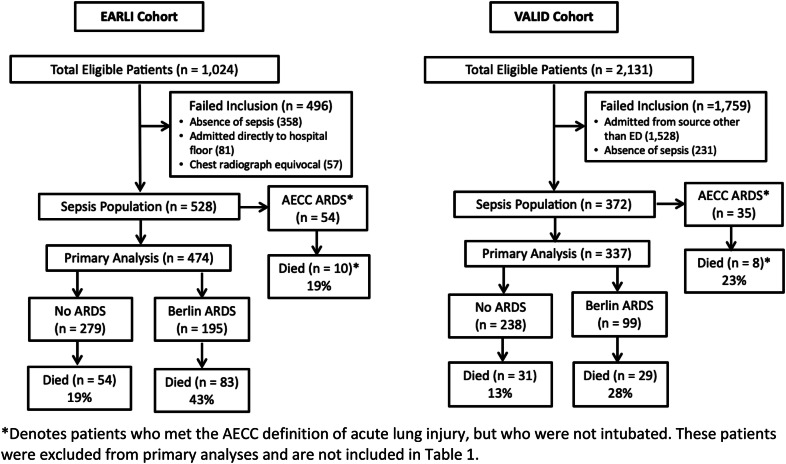
Methods: We studied two prospective sepsis cohorts drawn from the Early Assessment of Renal and Lung Injury (EARLI; n = 474) and Validating Acute Lung Injury markers for Diagnosis (VALID; n = 337) cohorts. ARDS was defined by Berlin criteria. We used logistic regression to compare in-hospital mortality in patients with and without ARDS, controlling for baseline severity of illness. We also estimated attributable mortality, adjusted for illness severity by stratification.
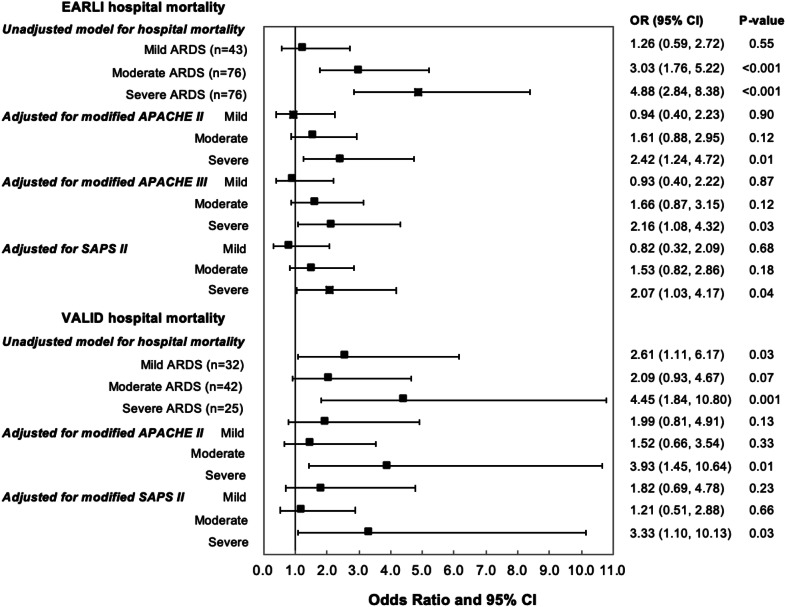
Results: ARDS occurred in 195 EARLI patients (41%) and 99 VALID patients (29%). ARDS was independently associated with risk of hospital death in multivariate analysis, even after controlling for severity of illness, as measured by APACHE II (odds ratio [OR] 1.65 (95% confidence interval [CI] 1.02, 2.67), p = 0.04 in EARLI; OR 2.12 (CI 1.16, 3.92), p = 0.02 in VALID). Patients with severe ARDS (P/F < 100) primarily drove this relationship. The attributable mortality of ARDS was 27% (CI 14%, 37%) in EARLI and 37% (CI 10%, 51%) in VALID. ARDS was independently associated with ICU mortality, hospital length of stay (LOS), ICU LOS, and ventilator-free days.
Conclusions: Development of ARDS among ICU patients with sepsis confers increased risk of ICU and in-hospital mortality in addition to other important outcomes. Clinical trials targeting patients with severe ARDS will be best poised to detect measurable differences in these outcomes.
Keywords: Acute lung injury; Acute respiratory distress syndrome; Mortality; Sepsis.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
Comment in
-
The attributable mortality of acute respiratory distress syndrome.Intensive Care Med. 2020 Jul;46(7):1508-1509. doi: 10.1007/s00134-020-06053-y. Epub 2020 Apr 27. Intensive Care Med. 2020. PMID: 32338308 No abstract available.
-
The attributable mortality of acute respiratory distress syndrome.Intensive Care Med. 2020 Jul;46(7):1510-1511. doi: 10.1007/s00134-020-06099-y. Epub 2020 May 25. Intensive Care Med. 2020. PMID: 32451576 Free PMC article. No abstract available.
References
-
- The Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
