

Cardiac arrhythmias in Dravet syndrome: an observational multicenter study
- PMID: 32207228
- PMCID: PMC7187713
- DOI: 10.1002/acn3.51017
Cardiac arrhythmias in Dravet syndrome: an observational multicenter study
Abstract
Objectives: We ascertained the prevalence of ictal arrhythmias to explain the high rate of sudden unexpected death in epilepsy (SUDEP) in Dravet syndrome (DS).
Methods: We selected cases with clinical DS, ≥6 years, SCN1A mutation, and ≥1 seizure/week. Home-based ECG recordings were performed for 20 days continuously. Cases were matched for age and sex to two epilepsy controls with no DS and ≥1 major motor seizure during video-EEG. We determined the prevalence of peri-ictal asystole, bradycardia, QTc changes, and effects of convulsive seizures (CS) on heart rate, heart rate variability (HRV), and PR/QRS. Generalized estimating equations were used to account for multiple seizures within subjects, seizure type, and sleep/wakefulness.
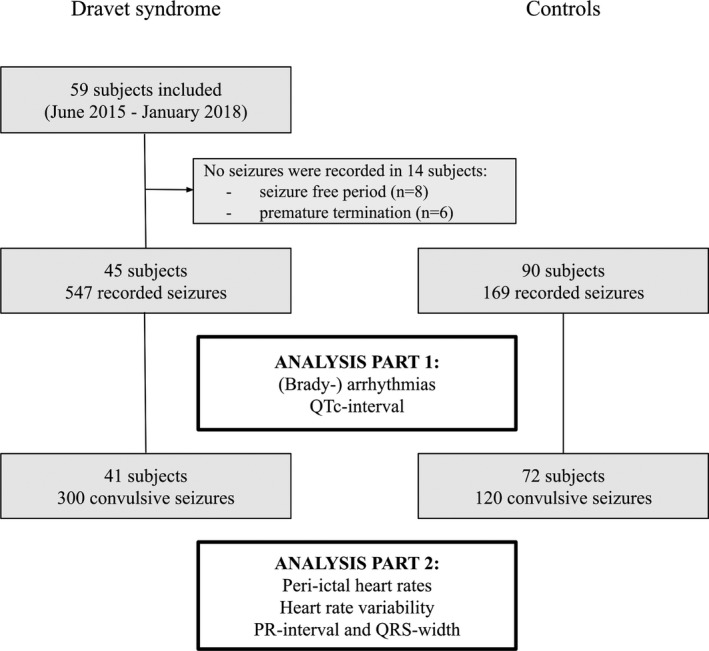
Results: We included 59 cases. Ictal recordings were obtained in 45 cases and compared to 90 controls. We analyzed 547 seizures in DS (300 CS) and 169 in controls (120 CS). No asystole occurred. Postictal bradycardia was more common in controls (n = 11, 6.5%) than cases (n = 4, 0.7%; P = 0.002). Peri-ictal QTc-lengthening (≥60ms) occurred more frequently in DS (n = 64, 12%) than controls (n = 8, 4.7%, P = 0.048); pathologically prolonged QTc was rare (once in each group). In DS, interictal HRV was lower compared to controls (RMSSD P = 0.029); peri-ictal values did not differ between the groups. Prolonged QRS/PR was rare and more common in controls (QRS: one vs. none; PR: three vs. one).
Interpretation: We did not identify major arrhythmias in DS which can directly explain high SUDEP rates. Peri-ictal QTc-lengthening was, however, more common in DS. This may reflect unstable repolarization and an increased propensity for arrhythmias.
© 2020 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals, Inc on behalf of American Neurological Association.
Conflict of interest statement
RS reports personal fees from UCB Pharma, EISAI, Cyberonics, Bial, Desitin, and LivaNova, RS is member of the editorial board of Epilepsy and Behavior and Epilepsia Open. JWS reports personal fees from UCB and Zogenix, grants from UCB, Eisai, UCB, GW Pharma. JWS's current position is endowed by the Epilepsy Society, he is a member of the Editorial Board of the Lancet Neurology and receives research support from the Marvin Weil Epilepsy Research Fund. JHC reports grants from GW Pharma, Zogenix, Marinius, Vitaflo, Nutricia, and National Institute for Health Research Biomedical Centre at Great Ormond Street Hospital for Children NHS Foundation trust. SS reports personal fees from UK Epilepsy Society. BG reports personal fees from GW Pharmaceuticals, Zogenix, and OVID/Takeda. RDT reports personal fees from UCB, GSK, Theravance, Novartis and Medtronic and grants from Nuts OHRA Foundation, Medtronic, AC Thomson Foundation and The Netherlands Organisation for Health Research and Development (ZonMW). RDT is a member of the editorial board of Seizure, Epilepsia and Clinical Autonomic Research. The remaining authors have no conflicts of interest relevant to this research.
Figures
References
-
- Cooper MS, McIntosh A, Crompton DE, et al. Mortality in Dravet syndrome. Epilepsy Res 2016;128:43–47. - PubMed
-
- Shmuely S, Sisodiya SM, Gunning WB, et al. Mortality in Dravet syndrome: a review. Epilepsy Behav 2016;64(Pt A):69–74. - PubMed
-
- Depienne C, Trouillard O, Saint‐Martin C, et al. Spectrum of SCN1A gene mutations associated with Dravet syndrome: analysis of 333 patients. J Med Genet 2009;46:183–191. - PubMed
-
- Marini C, Mei D, Temudo T, et al. Idiopathic epilepsies with seizures precipitated by fever and SCN1A abnormalities. Epilepsia 2007;48:1678–1685. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials