

Immediate and delayed autologous abdominal microvascular flap breast reconstruction in patients receiving adjuvant, neoadjuvant or no radiotherapy: a meta-analysis of clinical and quality-of-life outcomes
- PMID: 32207573
- PMCID: PMC7093792
- DOI: 10.1002/bjs5.50245
Immediate and delayed autologous abdominal microvascular flap breast reconstruction in patients receiving adjuvant, neoadjuvant or no radiotherapy: a meta-analysis of clinical and quality-of-life outcomes
Abstract
Background: Effects of postmastectomy radiotherapy (PMRT) on autologous breast reconstruction (BRR) are controversial regarding surgical complications, cosmetic appearance and quality of life (QOL). This systematic review evaluated these outcomes after abdominal free flap reconstruction in patients undergoing postoperative adjuvant radiotherapy (PMRT), preoperative radiotherapy (neoadjuvant radiotherapy) and no radiotherapy, aiming to establish evidence-based optimal timings for radiotherapy and BRR to guide contemporary management.
Methods: The study was registered on PROSPERO (CRD42017077945). Embase, MEDLINE, Google Scholar, CENTRAL, Science Citation Index and ClinicalTrials.gov were searched (January 2000 to August 2018). Study quality and risk of bias were assessed using GRADE and Cochrane's ROBINS-I respectively.
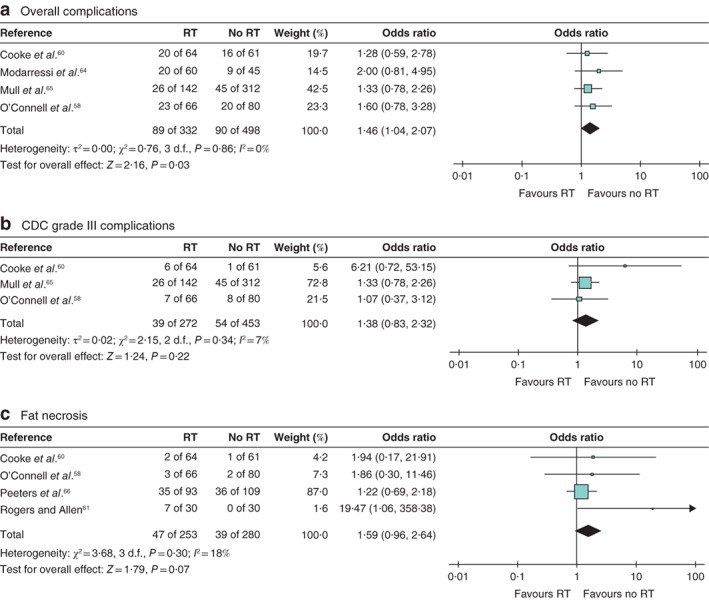
Results: Some 12 studies were identified, involving 1756 patients (350 PMRT, 683 no radiotherapy and 723 neoadjuvant radiotherapy), with a mean follow-up of 27·1 (range 12·0-54·0) months for those having PMRT, 16·8 (1·0-50·3) months for neoadjuvant radiotherapy, and 18·3 (1·0-48·7) months for no radiotherapy. Three prospective and nine retrospective cohorts were included. There were no randomized studies. Five comparative radiotherapy studies evaluated PMRT and four assessed neoadjuvant radiotherapy. Studies were of low quality, with moderate to serious risk of bias. Severe complications were similar between the groups: PMRT versus no radiotherapy (92 versus 141 patients respectively; odds ratio (OR) 2·35, 95 per cent c.i. 0·63 to 8·81, P = 0·200); neoadjuvant radiotherapy versus no radiotherapy (180 versus 392 patients; OR 1·24, 0·76 to 2·04, P = 0·390); and combined PMRT plus neoadjuvant radiotherapy versus no radiotherapy (272 versus 453 patients; OR 1·38, 0·83 to 2·32, P = 0·220). QOL and cosmetic studies used inconsistent methodologies.
Conclusion: Evidence is conflicting and study quality was poor, limiting recommendations for the timing of autologous BRR and radiotherapy. The impact of PMRT and neoadjuvant radiotherapy appeared to be similar.
Antecedentes: En pacientes sometidas a una reconstrucción mamaria (breast reconstruction, BRR) con tejido autólogo se discuten los efectos de la radioterapia post-mastectomía (post-mastectomy radiotherapy, PMRT) en las complicaciones quirúrgicas, el resultado estético y la calidad de vida (quality of life, QOL). Esta revisión sistemática evaluó dichos resultados tras una reconstrucción mamaria con un colgajo libre abdominal en pacientes tratadas con PMRT, radioterapia preoperatoria (Neo RT) y sin radioterapia (RT), a fin de establecer los momentos óptimos de la RT y BRR basados en la evidencia, como guía del tratamiento actual. MÉTODOS: El estudio se registró en la base de datos PROSPERO (CRD42017077945). Se realizaron búsquedas en Embase, MEDLINE, Google Scholar, CENTRAL, Science Citation Index y Clinicaltrials.gov (enero de 2000-agosto de 2018). La calidad de los estudios y el riesgo de sesgo se evaluaron mediante las herramientas GRADE y ROBINS-I de la Cochrane, respectivamente.
Resultados: Se identificaron 12 estudios que incluían 1.756 pacientes (350 PMRT, 683 sin RT y 723 Neo RT), con una mediana de seguimiento de 27,1 meses (rango 12,0-54,0) para PMRT, 16,8 meses (1,0-50,3) para Neo RT y 18,3 meses (1,0-48,7) para sin RT. Se incluyeron tres cohortes prospectivas y nueve retrospectivas. No hubo estudios aleatorizados. Los estudios comparativos de RT evaluaron la PMRT (n = 5) y la Neo RT (n = 4). Todos los estudios fueron de baja calidad, con riesgos de sesgo de moderados a graves. Las complicaciones graves fueron similares entre los grupos: PMRT (n = 92) versus sin RT (n = 141), razón de oportunidades (odds ratio, OR) 2,35, i.c. del 95% 0,63-8,81), P = 0,200; Neo RT (n = 180) versus no RT (n = 392) (OR 1,24, i.c. del 95% 0,76-2,04), P = 0,390; o RT combinada (PMRT y neoadyuvante) (n = 272) versus no RT (n = 453) (OR 1,38, i.c. del 95% 0,83-2,32), P = 0,220. Los estudios de calidad de vida y de resultados estéticos utilizaron metodologías poco consistentes. CONCLUSIÓN: La evidencia es contradictoria y la calidad de los estudios muy pobre, hechos que limitan las posibles recomendaciones para el momento de la BRR con tejido autólogo y la RT. El impacto de la PMRT o la Neo RT parecen ser similares.
© 2019 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures



References
-
- Winters S, Martin C, Murphy D, Shokar NK. Breast cancer epidemiology, prevention, and screening. Prog Mol Biol Transl Sci 2017; 151: 1–32. - PubMed
-
- Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A et al Twenty‐year follow‐up of a randomized study comparing breast‐conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 2002; 347: 1227–1232. - PubMed
-
- van Maaren MC, le Cessie S, Strobbe LJA, Groothuis‐Oudshoorn CGM, Poortmans PMP, Siesling S. Different statistical techniques dealing with confounding in observational research: measuring the effect of breast‐conserving therapy and mastectomy on survival. J Cancer Res Clin Oncol 2019; 145: 1485–1493. - PMC - PubMed
-
- Ho AY, Hu ZI, Mehrara BJ, Wilkins EG. Radiotherapy in the setting of breast reconstruction: types, techniques, and timing. Lancet Oncol 2017; 18: e742–e753. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
