

Impact of single versus double transseptal puncture on outcome and complications in pulmonary vein isolation procedures
- PMID: 32207839
- PMCID: PMC8428934
- DOI: 10.5603/CJ.a2020.0037
Impact of single versus double transseptal puncture on outcome and complications in pulmonary vein isolation procedures
Abstract
Background: The aim of the current study was to analyze the impact of single versus double transseptal puncture (TSP) for atrial fibrillation (AF) ablation.
Methods: Consecutive patients undergoing AF ablation were prospectively included in the AF ablation registry and were analyzed according to single versus double TSP.
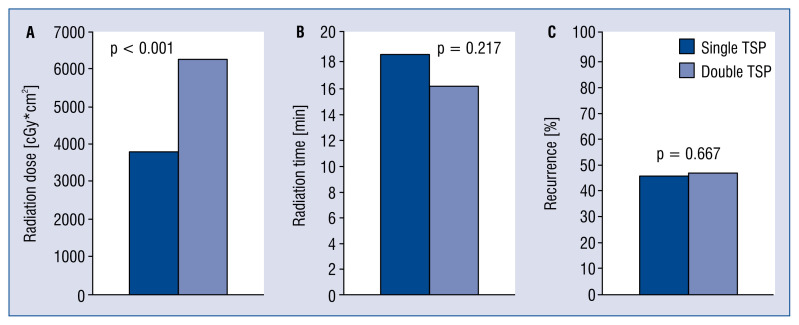
Results: A total of 478 patients (female 35%, persistent AF 67%) undergoing AF ablation between 01/2014 and 09/2014 were included. Single TSP was performed in 202 (42%) patients, double TSP in 276 (58%) patients. Age, gender, body mass index, CHA2DS2-VASc score, left ventricular ejection fraction and operator experience (experienced operator defined as ≥ 5 years of experience in invasive electrophysiology) were equally distributed between the two groups. Repeat procedures (re-dos) were more frequently performed using single TSP access (p < 0.001). Left atrial (LA) diameter was larger in patients with double TSP (p = 0.001). Procedure duration in single TSP was identical to double TSP procedures (p = 0.823). Radiation duration was similar between the two groups (p = 0.217). There were 49 (10%) patients with complications after catheter ablation. There were no differences between complication rates and TSP type (p = 0.555). Similarly, recurrence rates were comparable between both TSP groups (p = 0.788).
Conclusions: There was no clear benefit of single or double TSP in AF ablation.
Keywords: atrial fibrillation; catheter ablation; complications; pulmonary vein isolation; transseptal puncture.
Conflict of interest statement
Figures
Similar articles
-
A simplified single transseptal puncture approach using high-density 3D voltage mapping for atrial fibrillation ablation: acute complications and long-term results.Front Cardiovasc Med. 2023 Nov 23;10:1309900. doi: 10.3389/fcvm.2023.1309900. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38075955 Free PMC article.
-
Bailout Atrial Balloon Septoplasty to Overcome Challenging Left Atrial Transseptal Access for Catheter Ablation of Atrial Fibrillation.JACC Clin Electrophysiol. 2018 Aug;4(8):1011-1019. doi: 10.1016/j.jacep.2018.04.003. Epub 2018 May 30. JACC Clin Electrophysiol. 2018. PMID: 30139482
-
Remote-controlled magnetic pulmonary vein isolation using a new three-dimensional non-fluoroscopic navigation system: a single-centre prospective study.Arch Cardiovasc Dis. 2013 Aug-Sep;106(8-9):423-32. doi: 10.1016/j.acvd.2013.04.008. Epub 2013 Jul 29. Arch Cardiovasc Dis. 2013. PMID: 23906679
-
Transseptal Access to the Left Atrium: Tips and Tricks to Keep it Safe Derived from Single Operator Experience and Review of the Literature.Curr Cardiol Rev. 2017;13(4):305-318. doi: 10.2174/1573403X13666170927122036. Curr Cardiol Rev. 2017. PMID: 28969539 Free PMC article. Review.
-
Safety and efficacy of catheter ablation for atrial fibrillation in patients with percutaneous atrial septal closure device: Electrophysiology Collaborative Consortium for Meta-analysis-ELECTRAM Investigators.J Cardiovasc Electrophysiol. 2020 Sep;31(9):2328-2334. doi: 10.1111/jce.14616. Epub 2020 Jun 25. J Cardiovasc Electrophysiol. 2020. PMID: 32530528
Cited by
-
2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation.J Interv Card Electrophysiol. 2024 Aug;67(5):921-1072. doi: 10.1007/s10840-024-01771-5. J Interv Card Electrophysiol. 2024. Corrected and republished in: Heart Rhythm. 2024 Sep;21(9):e31-e149. doi: 10.1016/j.hrthm.2024.03.017. PMID: 38609733 Corrected and republished.
-
Single puncture approach guided by transesophageal echocardiography for atrial fibrillation ablation in a patient with prior percutaneous septal closure: case report.Eur Heart J Case Rep. 2023 Apr 12;7(4):ytad139. doi: 10.1093/ehjcr/ytad139. eCollection 2023 Apr. Eur Heart J Case Rep. 2023. PMID: 37090759 Free PMC article.
-
Best practices in robotic magnetic navigation-guided catheter ablation of cardiac arrhythmias, a position paper of the Society for Cardiac Robotic Navigation.Front Cardiovasc Med. 2024 Sep 27;11:1431396. doi: 10.3389/fcvm.2024.1431396. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39399515 Free PMC article. Review.
-
2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation.Europace. 2024 Mar 30;26(4):euae043. doi: 10.1093/europace/euae043. Europace. 2024. Corrected and republished in: Heart Rhythm. 2024 Sep;21(9):e31-e149. doi: 10.1016/j.hrthm.2024.03.017. PMID: 38587017 Free PMC article. Corrected and republished.
-
2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation.J Arrhythm. 2024 Oct 6;40(6):1217-1354. doi: 10.1002/joa3.13082. eCollection 2024 Dec. J Arrhythm. 2024. PMID: 39669937 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
