

Innate and adaptive immune cell subsets as risk factors for coronary heart disease in two population-based cohorts
- PMID: 32209232
- PMCID: PMC7276206
- DOI: 10.1016/j.atherosclerosis.2020.03.011
Innate and adaptive immune cell subsets as risk factors for coronary heart disease in two population-based cohorts
Abstract
Background and aims: Cell-mediated immunity is implicated in atherosclerosis. We evaluated whether innate and adaptive immune cell subsets in peripheral blood are risk factors for coronary heart disease.
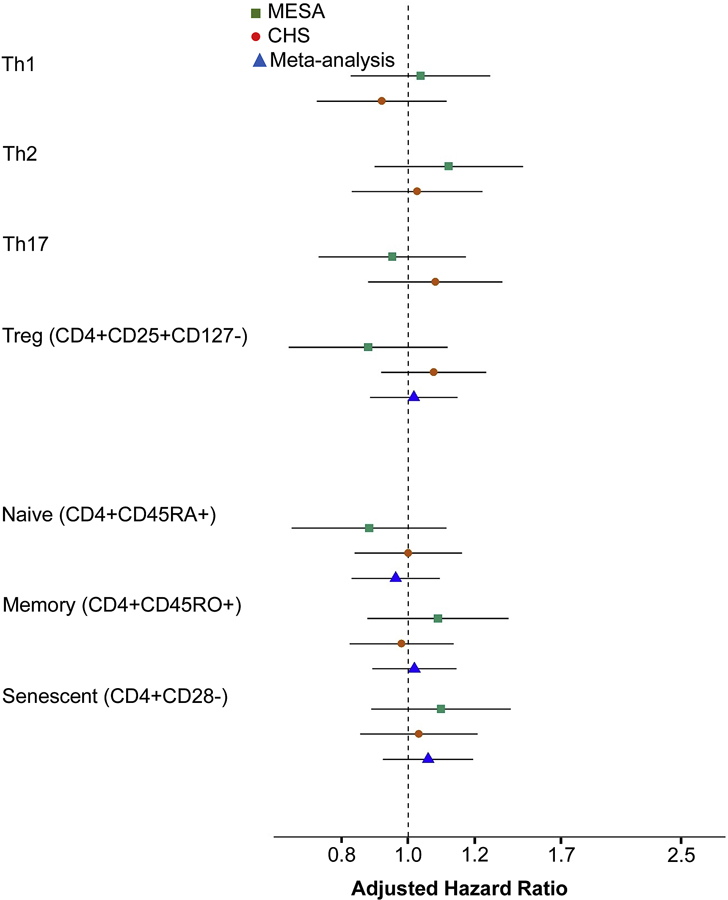
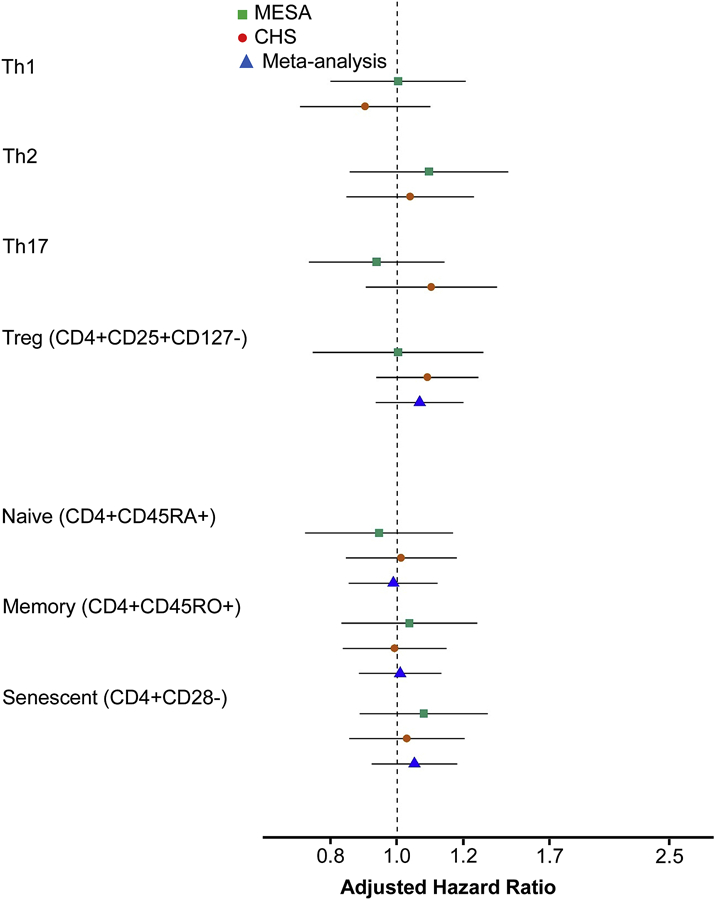
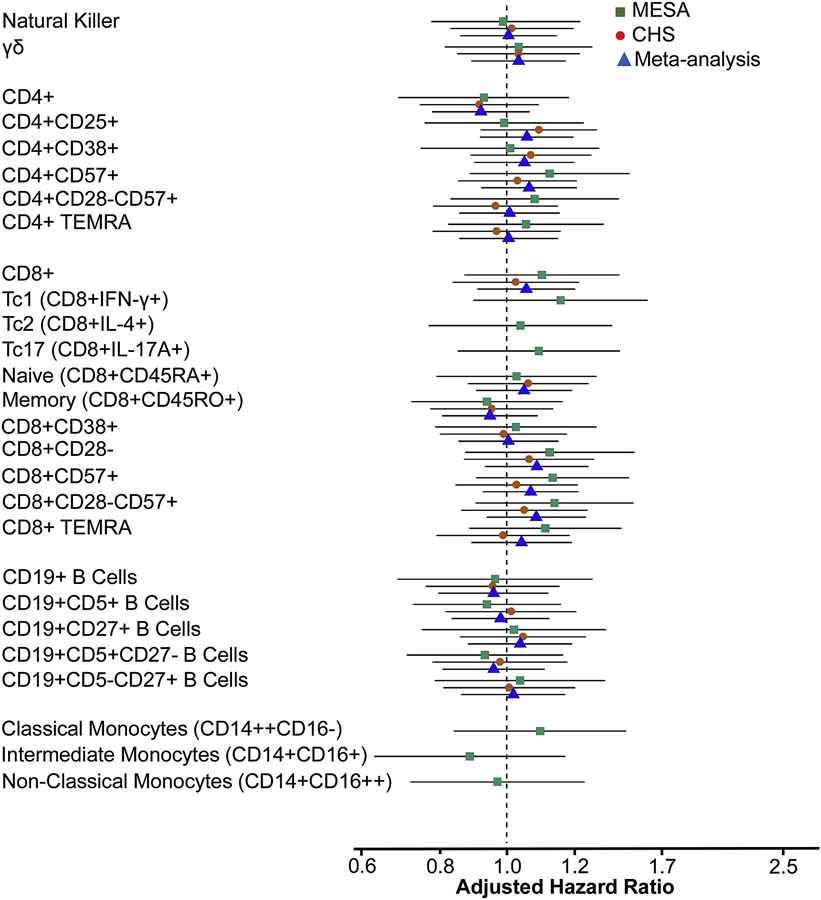
Methods: A nested case-cohort study (n = 2155) was performed within the Multi-Ethnic Study of Atherosclerosis (MESA) and the Cardiovascular Health Study (CHS). Cases of incident myocardial infarction (MI) and incident angina (n = 880 total cases) were compared with a cohort random sample (n = 1275). Immune cell phenotypes (n = 34, including CD14+ monocytes, natural killer cells, γδ T cells, CD4+, CD8+ and CD19+ lymphocyte subsets) were measured from cryopreserved cells by flow cytometry. Cox proportional hazards models with adjustment for cardiovascular disease risk factors were used to evaluate associations of cell phenotypes with incident MI and a composite phenotype of incident MI or incident angina (MI-angina) over a median 9.3 years of follow-up. Th1, Th2, Th17, T regulatory (CD4+CD25+CD127-), naive (CD4+CD45RA+), memory (CD4+CD45RO+), and CD4+CD28- cells were specified as primary hypotheses. In secondary analyses, 27 additional cell phenotypes were investigated.
Results: After correction for multiple testing, there were no statistically significant associations of CD4+ naive, memory, CD28-, or T helper cell subsets with MI or MI-angina in MESA, CHS, or combined-cohort meta analyses. Null associations were also observed for monocyte subsets, natural killer cells, γδ T cells, CD19+ B cell and differentiated CD4+ and CD8+ cell subsets.
Conclusions: The proportions of peripheral blood monocyte and lymphocyte subsets are not strongly related to the future occurrence of MI or angina in adults free of autoimmune disease.
Keywords: Biomarkers; Cardiovascular disease; Immunity; Inflammation; Risk factors; T cells.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Gistera A and Hansson GK, The immunology of atherosclerosis. Nat Rev Nephrol, 2017. 13(6): p. 368–380. - PubMed
-
- Huber SA, et al., T helper-cell phenotype regulates atherosclerosis in mice under conditions of mild hypercholesterolemia. Circulation, 2001. 103(21): p. 2610–6. - PubMed
-
- Nour-Eldine W, et al., Genetic Depletion or Hyperresponsiveness of Natural Killer Cells Do Not Affect Atherosclerosis Development. Circ Res, 2018. 122(1): p. 47–57. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- R00 HL129045/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- R01 HL120854/HL/NHLBI NIH HHS/United States
- R01 HL135625/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
