

Abdominal and pelvic radiographs of medical devices and materials- part 2: neurologic and genitourinary devices and materials
- PMID: 32209503
- PMCID: PMC7239358
- DOI: 10.5152/dir.2019.19391
Abdominal and pelvic radiographs of medical devices and materials- part 2: neurologic and genitourinary devices and materials
Abstract
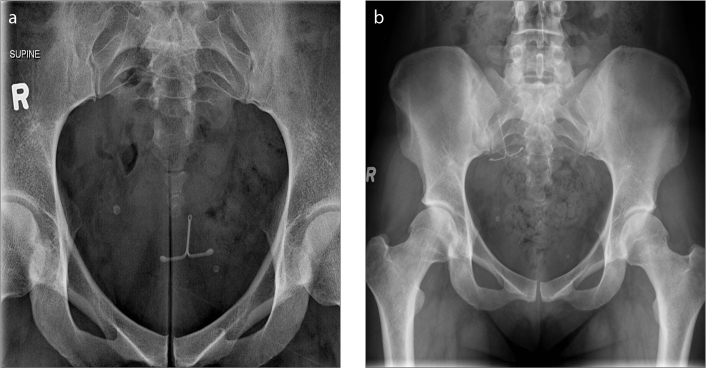
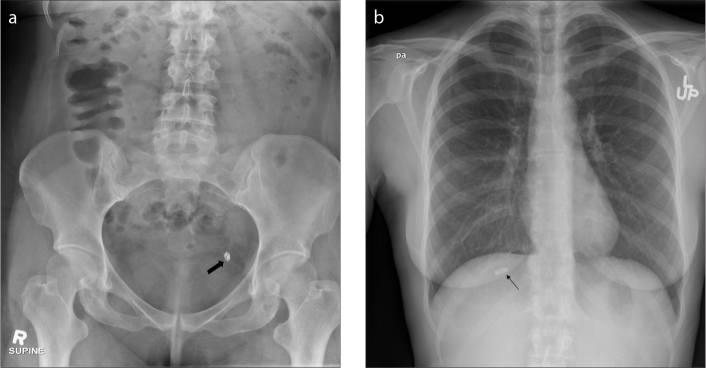
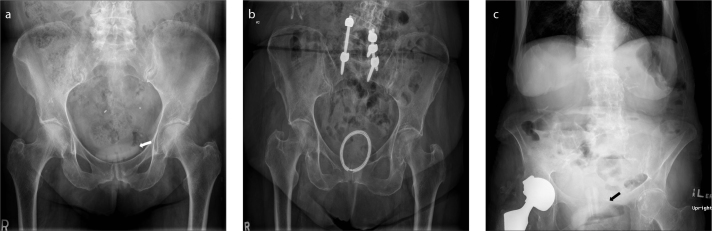
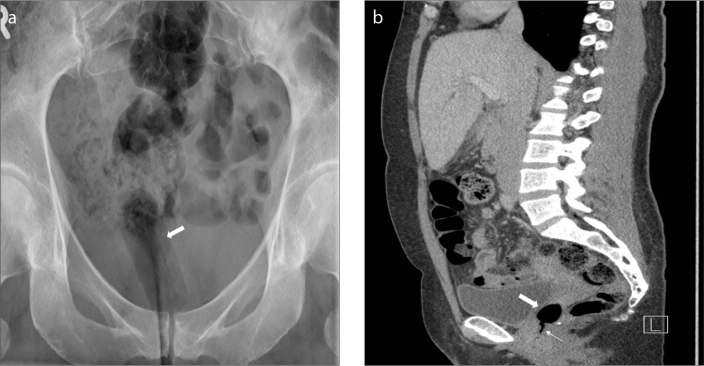
Radiographs of the abdomen and pelvis are routinely obtained as a standard part of clinical care for the abdomen and pelvis. Brisk advances in technology over the last few decades have resulted in a multitude of medical devices and materials. Recognizing and evaluating these devices on abdominal and pelvic radiographs are critical, yet increasingly a difficult endeavor. In addition, multiple devices serving different purposes may have a similar radiographic appearance and position causing confusion for the interpreting radiologist. The role of the radiologist is to not only identify accurately these medical objects, but also to confirm for their accurate placement and to recognize any complications that could affect patient care, management or even be potentially life threatening. An extensive online search of literature showed our review article to be the most comprehensive work on medical devices and materials of the abdomen and pelvis, and in this second part of our two-part series, we discuss in depth about the neurologic and genitourinary devices seen on abdominal and pelvic radiographs.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures







Similar articles
-
Abdominal and pelvic radiographs of medical devices and materials-Part 1: gastrointestinal and vascular devices and materials.Diagn Interv Radiol. 2020 Mar;26(2):101-110. doi: 10.5152/dir.2019.19390. Diagn Interv Radiol. 2020. PMID: 32071024 Free PMC article. Review.
-
Imaging of abdominal and pelvic surgical and postprocedural foreign bodies.Radiol Clin North Am. 2014 Sep;52(5):991-1027. doi: 10.1016/j.rcl.2014.05.006. Radiol Clin North Am. 2014. PMID: 25173655 Review.
-
Misplaced devices in the chest, abdomen, and pelvis: Part II.Semin Ultrasound CT MR. 2006 Apr;27(2):98-110. doi: 10.1053/j.sult.2006.01.003. Semin Ultrasound CT MR. 2006. PMID: 16623364 Review.
-
Misplaced devices in the chest, abdomen, and pelvis: Part I.Semin Ultrasound CT MR. 2006 Apr;27(2):78-97. doi: 10.1053/j.sult.2006.01.002. Semin Ultrasound CT MR. 2006. PMID: 16623363 Review.
-
Medical devices of the abdomen and pelvis.Radiographics. 2005 Mar-Apr;25(2):503-23. doi: 10.1148/rg.252045157. Radiographics. 2005. PMID: 15798067
Cited by
-
Misidentification of Medical Devices With Radiographic Contrast Functions As Retained Foreign Bodies on Postoperative Radiographs: A Report of Two Cases.Cureus. 2025 Jan 28;17(1):e78154. doi: 10.7759/cureus.78154. eCollection 2025 Jan. Cureus. 2025. PMID: 40027052 Free PMC article.
-
A multimodality review of gynecologic devices in the pelvis.Abdom Radiol (NY). 2024 Jul;49(7):2459-2477. doi: 10.1007/s00261-024-04367-9. Epub 2024 May 28. Abdom Radiol (NY). 2024. PMID: 38805098 Review.
References
-
- Kalia V, Bizzell C, Obray R, Obray J, Lamer T, Carrino JA. Spinal cord stimulation: the types of neurostimulation devices currently being used, and what radiologists need to know when evaluating their appearance on imaging. Curr Probl Diagn Radiol. 2010;39:227–233. doi: 10.1067/j.cpradiol.2009.07.010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
