

Survival after checkpoint inhibitors for metastatic acral, mucosal and uveal melanoma
- PMID: 32209601
- PMCID: PMC7103823
- DOI: 10.1136/jitc-2019-000341
Survival after checkpoint inhibitors for metastatic acral, mucosal and uveal melanoma
Abstract
Background: Checkpoint inhibitors (CPIs) are thought to be effective against cutaneous melanoma in part because of the large burden of somatic mutations (neoantigens) generated from exposure to ultraviolet radiation. However, rare melanoma subtypes arising from acral skin, mucosal surfaces, and the uveal tract are largely sun-shielded. Genomic studies show these sun-shielded melanomas have a paucity of neoantigens and unique biology; they are thought to be largely resistant to immunotherapy. It has not been definitively shown that CPI improves survival in metastatic sun-shielded melanoma.
Methods: We reviewed a single institutional experience using antibodies against CTLA-4, PD-1 and/or PD-L1 to treat patients with metastatic melanoma. Primary tumor histology was categorized as cutaneous, unknown, acral, mucosal, or uveal. We studied demographic data, treatment characteristics, and overall survival (OS) after CPI.
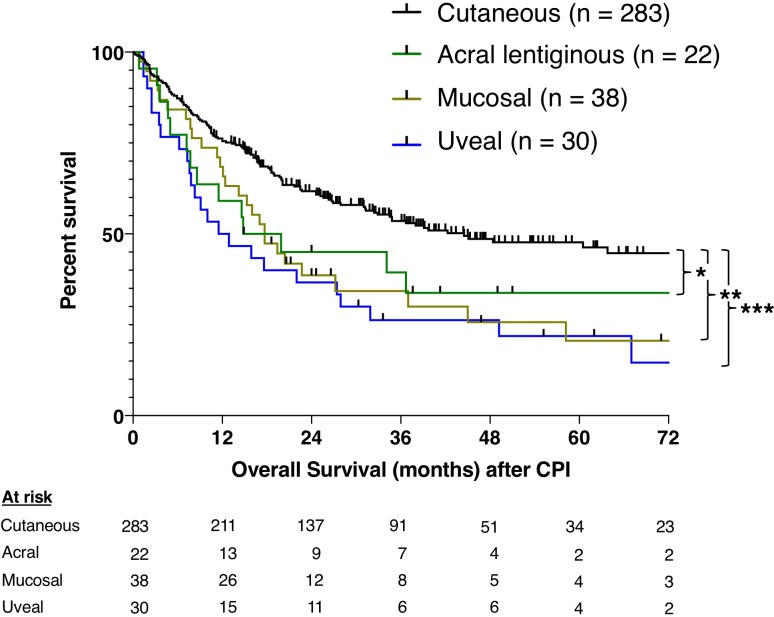
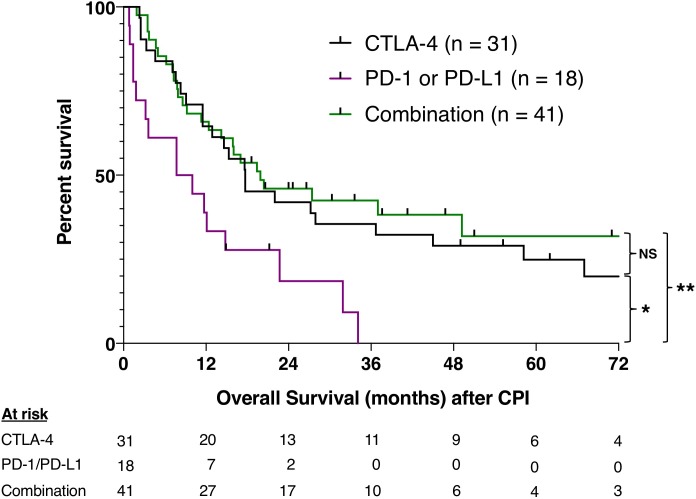
Results: We treated 428 patients with metastatic melanoma from 2007 to 2019. Primary tumors were cutaneous in 283 (66%), unknown in 55 (13%), acral in 22 (5%), mucosal in 38 (9%), and uveal in 30 (7%). Patients with metastatic disease from cutaneous primary tumors had median OS after CPI of 45 months compared with 17 months for acral (p=0.047), 18 months for mucosal (p=0.003), and 12 months for uveal (p<0.001). For all patients with sun-shielded melanoma (n=90), first treatment with anti-PD-1 or anti-PD-L1 was followed by a median OS of 9 months compared with 18 months after anti-CTLA-4 (p=0.010) and 20 months after combination therapy (p=0.003). There were 21 patients who achieved actual 3-year survival; 20 received both anti-CTLA-4 and anti-PD-1, either sequentially or in combination. Over 80% of 3-year survivors with progressive disease were treated with local therapy after CPI.
Conclusions: Long survival in patients with metastatic melanoma from acral, mucosal, and uveal primary tumors was associated with receipt of both anti-CTLA-4 and anti-PD-1 antibodies. Complete responses were rare, and local therapy was frequently employed to control disease progression. While sun-shielded melanomas exhibit worse outcomes after CPI than cutaneous melanomas, with an aggressive multidisciplinary approach, 5-year survival is still possible for 25%-32% of these patients.
Keywords: acral lentiginous melanoma; checkpoint inhibitors; immunotherapy; melanoma; mucosal melanoma; uveal melanoma.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: No, there are no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials