

Consensus guidelines for the definition, detection and interpretation of immunogenic cell death
- PMID: 32209603
- PMCID: PMC7064135
- DOI: 10.1136/jitc-2019-000337
Consensus guidelines for the definition, detection and interpretation of immunogenic cell death
Erratum in
-
Correction: Consensus guidelines for the definition, detection and interpretation of immunogenic cell death.J Immunother Cancer. 2020 May;8(1):e000337corr1. doi: 10.1136/jitc-2019-000337corr1. J Immunother Cancer. 2020. PMID: 32448801 Free PMC article. No abstract available.
Abstract
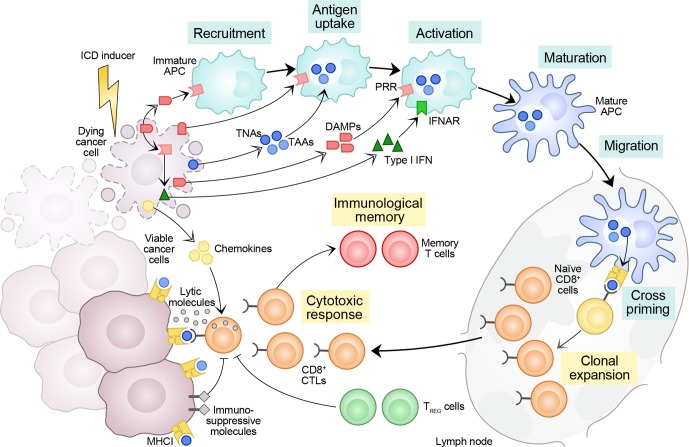
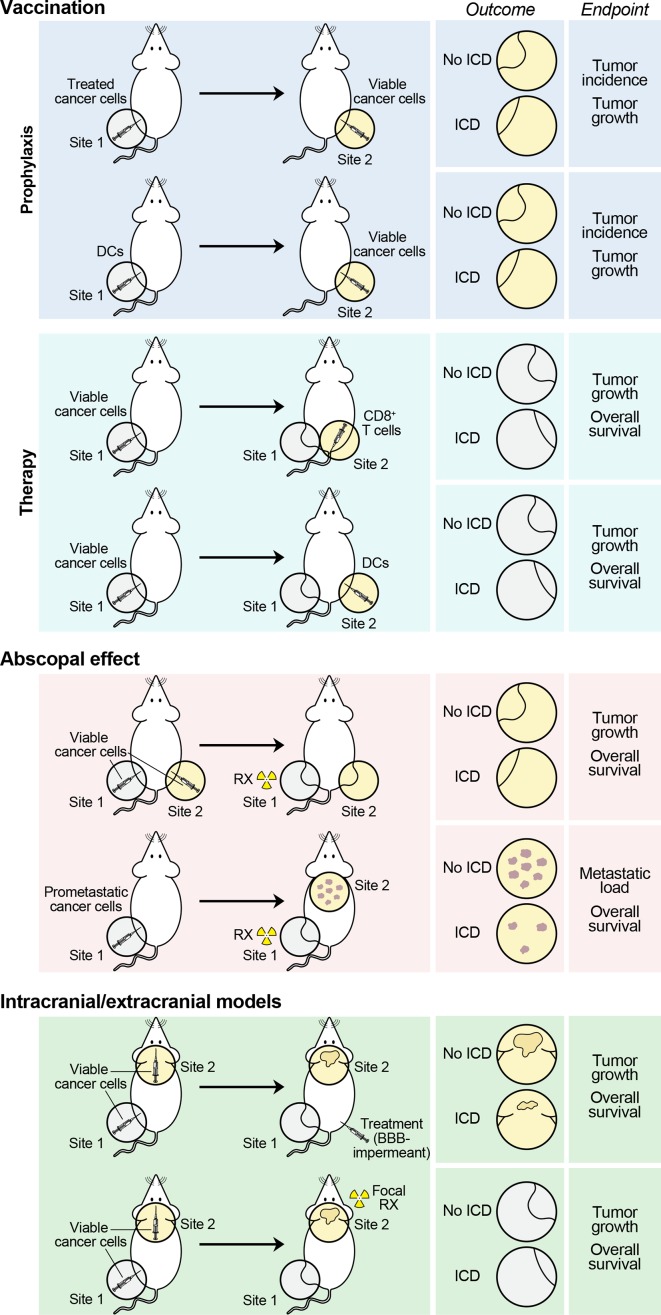
Cells succumbing to stress via regulated cell death (RCD) can initiate an adaptive immune response associated with immunological memory, provided they display sufficient antigenicity and adjuvanticity. Moreover, multiple intracellular and microenvironmental features determine the propensity of RCD to drive adaptive immunity. Here, we provide an updated operational definition of immunogenic cell death (ICD), discuss the key factors that dictate the ability of dying cells to drive an adaptive immune response, summarize experimental assays that are currently available for the assessment of ICD in vitro and in vivo, and formulate guidelines for their interpretation.
Keywords: immunology; molecular biology; oncology.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases