

Towards defining the surgical workforce for children: a geospatial analysis in Brazil
- PMID: 32209626
- PMCID: PMC7202732
- DOI: 10.1136/bmjopen-2019-034253
Towards defining the surgical workforce for children: a geospatial analysis in Brazil
Abstract
Objectives: The optimal size of the health workforce for children's surgical care around the world remains poorly defined. The goal of this study was to characterise the surgical workforce for children across Brazil, and to identify associations between the surgical workforce and measures of childhood health.
Design: This study is an ecological, cross-sectional analysis using data from the Brazil public health system (Sistema Único de Saúde).
Settings and participants: We collected data on the surgical workforce (paediatric surgeons, general surgeons, anaesthesiologists and nursing staff), perioperative mortality rate (POMR) and under-5 mortality rate (U5MR) across Brazil for 2015.
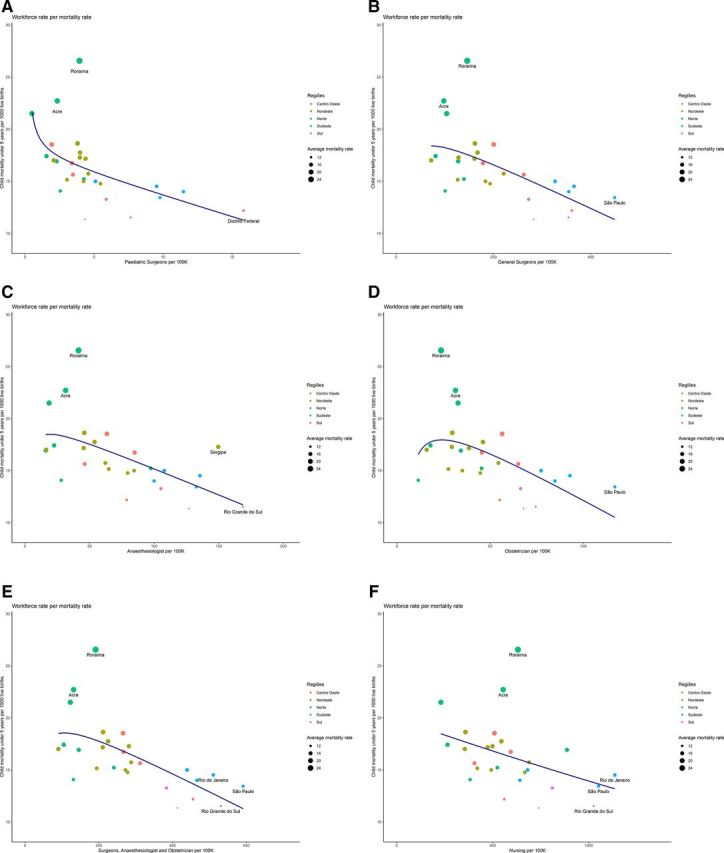
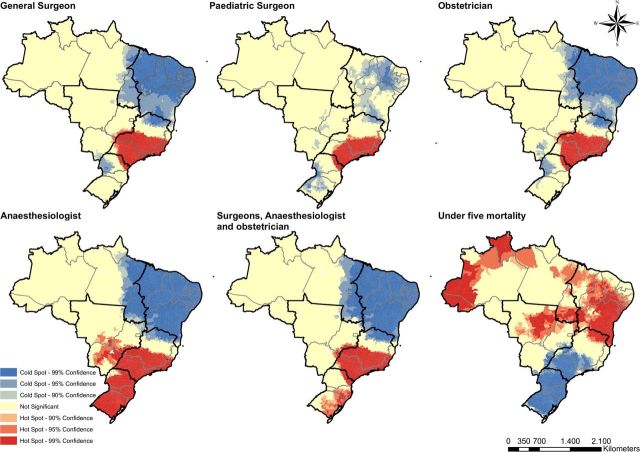
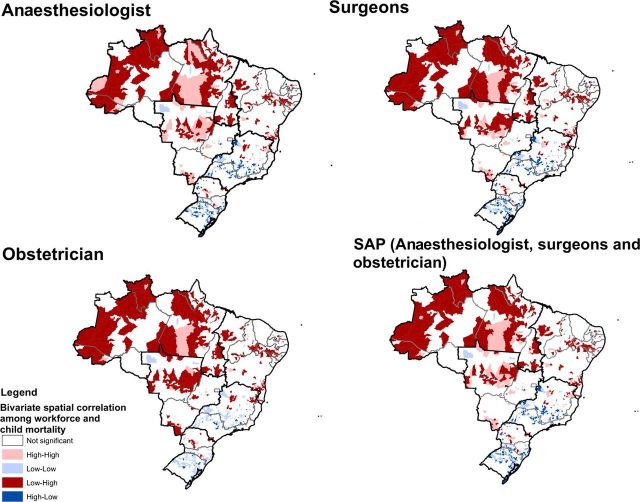
Primary and secondary outcome measures: We performed descriptive analyses, and identified associations between the workforce and U5MR using geospatial analysis (Getis-Ord-Gi analysis, spatial cluster analysis and linear regression models).
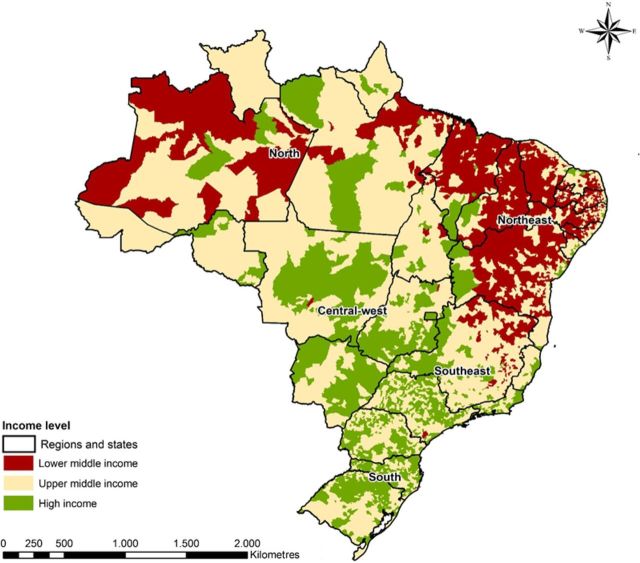
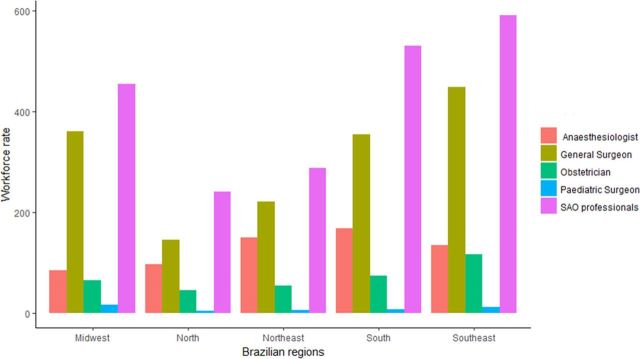
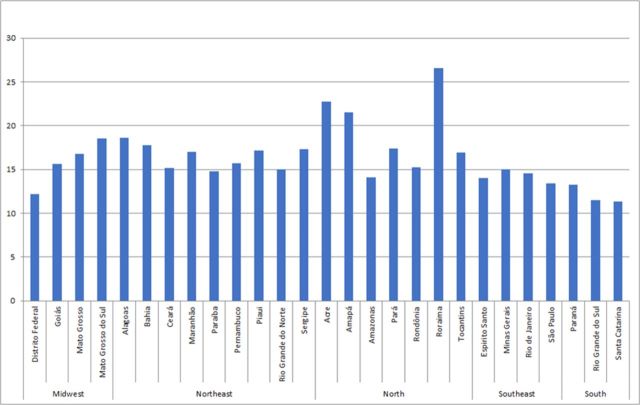
Findings: There were 39 926 general surgeons, 856 paediatric surgeons, 13 243 anaesthesiologists and 103 793 nurses across Brazil in 2015. The U5MR ranged from 11 to 26 deaths/1000 live births and the POMR ranged from 0.11-0.17 deaths/100 000 children across the country. The surgical workforce is inequitably distributed across the country, with the wealthier South and Southeast regions having a higher workforce density as well as lower U5MR than the poorer North and Northeast regions. Using linear regression, we found an inverse relationship between the surgical workforce density and U5MR. An U5MR of 15 deaths/1000 births across Brazil is associated with a workforce level of 5 paediatric surgeons, 200 surgeons, 100 anaesthesiologists or 700 nurses/100 000 children.
Conclusions: We found wide disparities in the surgical workforce and childhood mortality across Brazil, with both directly related to socioeconomic status. Areas of increased surgical workforce are associated with lower U5MR. Strategic investment in the surgical workforce may be required to attain optimal health outcomes for children in Brazil, particularly in rural regions.
Keywords: epidemiology; paediatrics; surgery.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical