

Haemorrhagic transformation following ischaemic stroke: A retrospective study
- PMID: 32210323
- PMCID: PMC7093519
- DOI: 10.1038/s41598-020-62230-5
Haemorrhagic transformation following ischaemic stroke: A retrospective study
Abstract
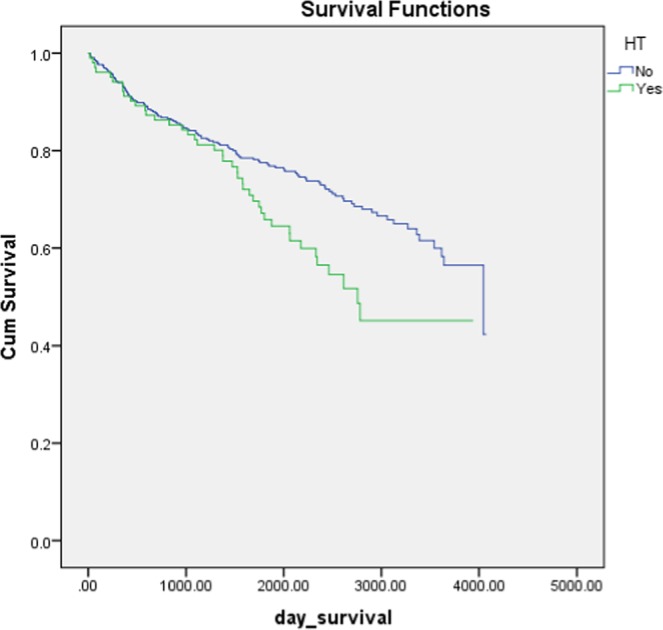
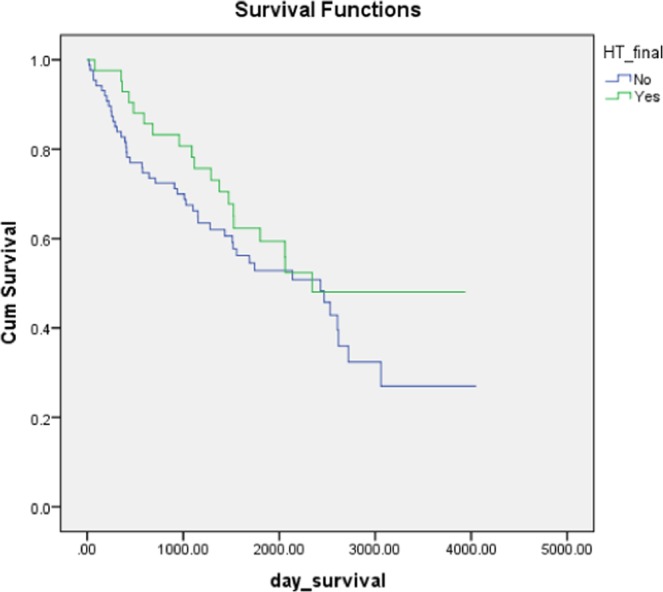
The aim of this study was to identify the prevalence of haemorrhagic transformation (HT) in patients with ischaemic stroke, and evaluate its association with medical comorbidities, stroke subtypes, premorbid medication, and long-term survival. To achieve this, we performed a retrospective analysis of 527 consecutive stroke rehabilitation patients. Of these, 102 (19.4%) developed HT. Older patients, and those with large artery strokes, had a higher risk of HT. Forty-one patients received alteplase (rtPA), of which 15 (36.6%) developed HT. A total of 129 (24.5%) patients were taking aspirin prior to their stroke and, of these, 39 (30.2%) developed HT. Twenty-three (4.36%) patients were taking vitamin k antagonists, prior to stroke, of which 14 (60.9%) developed HT. There were 102 patients (19.35%) with underlying atrial fibrillation, of whom 55 (53.9%) developed HT. Patients with known ischaemic heart disease had an increased risk of HT, and patients with HT had significantly lower total cholesterol levels (4.96 vs. 5.34) and lower LDL cholesterol levels (3.20 vs. 3.5). In conclusion, older age, atrial fibrillation, treatment with oral anticoagulants and antiplatelet medications prior to stroke, low total and LDL cholesterol, and rtPA use, are all associated with HT. Survival was not affected by the presence of HT.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Fisher M, Adams RD. Observation on brain embolism with special ref to the mechanism of haemorrhagic infarction. J. Neuropathol. Exp. Neuro. 1951;10:92–94. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
