

Impact of diabetes, obesity and hypertension on preterm birth: Population-based study
- PMID: 32210434
- PMCID: PMC7094836
- DOI: 10.1371/journal.pone.0228743
Impact of diabetes, obesity and hypertension on preterm birth: Population-based study
Abstract
Objective: To determine the impact of pre-pregnancy diabetes mellitus (D), obesity (O) and chronic hypertension (H) on preterm birth (PTB).
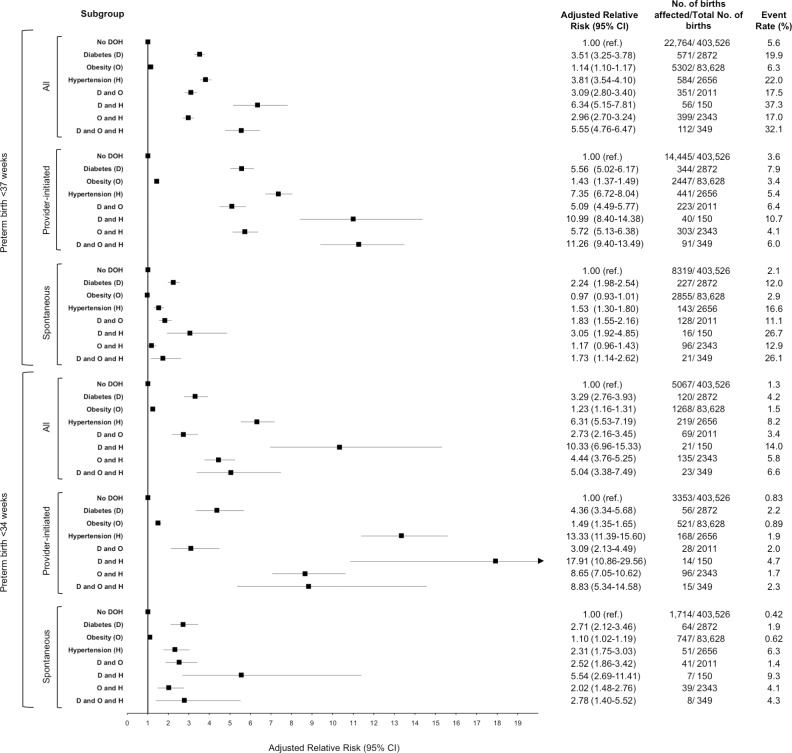
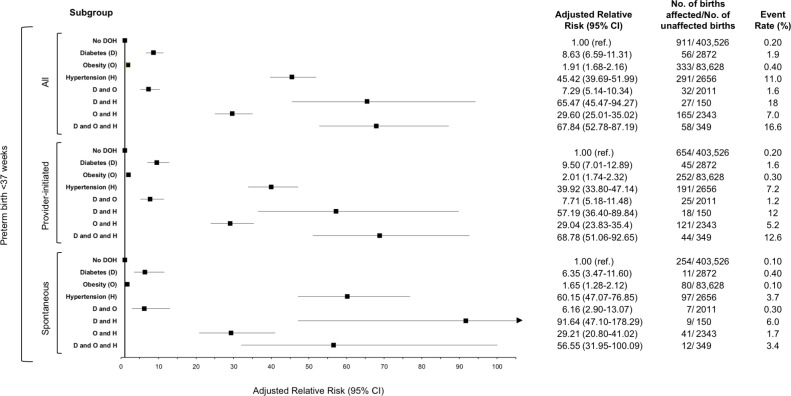
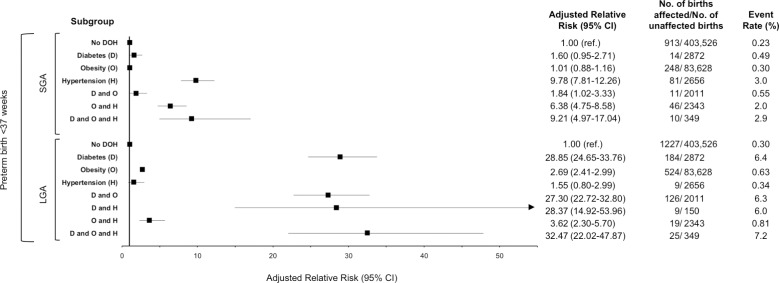
Methods: Retrospective population-based cohort study in Ontario, Canada between 2012-2016. Women who had a singleton livebirth or stillbirth at > 20 weeks gestation were included in the cohort. Exposures of interest were D, O and H, individually, and in various combinations. The primary outcome was PTB at 241/7 to 366/7 weeks. PTB was further analyzed by spontaneous or provider-initiated, early (< 34 weeks) or late (34-37 weeks), and the co-presence of preeclampsia, large for gestational age (LGA), and small for gestational age (SGA). Multivariable Poisson regression models with robust error variance were used to generate relative risks (RR), further adjusted for maternal age and parity (aRR). Population attributable fractions (PAF) were calculated for each of the outcomes by exposure state.
Results: 506,483 women were eligible for analysis. 30,139 pregnancies (6.0%) were complicated by PTB < 37 weeks, of which 7375 (24.5%) had D or O or H. Relative to women without D or O or H, the aRR for PTB < 37 weeks was higher for D (3.51; 95% CI 3.26-3.78) and H (3.81; 95% CI 3.55-4.10) than O (1.14; 95% CI 1.10-1.17). The combined state of DH was associated with a significantly higher aRR of PTB < 37 weeks (6.34; 95% CI 5.14-7.80) and < 34 weeks (aRR 10.33, 95% CI 6.96-15.33) than D alone. The risk of provider initiated PTB was generally higher than that for spontaneous PTB. Pre-pregnancy hypertension was associated with the highest risk for PTB with preeclampsia (aRR 45.42, 95% CI 39.69-51.99) and PTB with SGA (aRR 9.78, 95% CI 7.81-12.26) while pre-pregnancy diabetes was associated with increased risk for PTB with LGA (aRR 28.85, 95% CI 24.65-33.76).
Conclusion: Combinations of DOH significantly magnify the risk of PTB, especially provider initiated PTB, and PTB with altered fetal growth or preeclampsia.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
