

Bone mineral density changes among people living with HIV who have started with TDF-containing regimen: A five-year prospective study
- PMID: 32210458
- PMCID: PMC7094833
- DOI: 10.1371/journal.pone.0230368
Bone mineral density changes among people living with HIV who have started with TDF-containing regimen: A five-year prospective study
Abstract
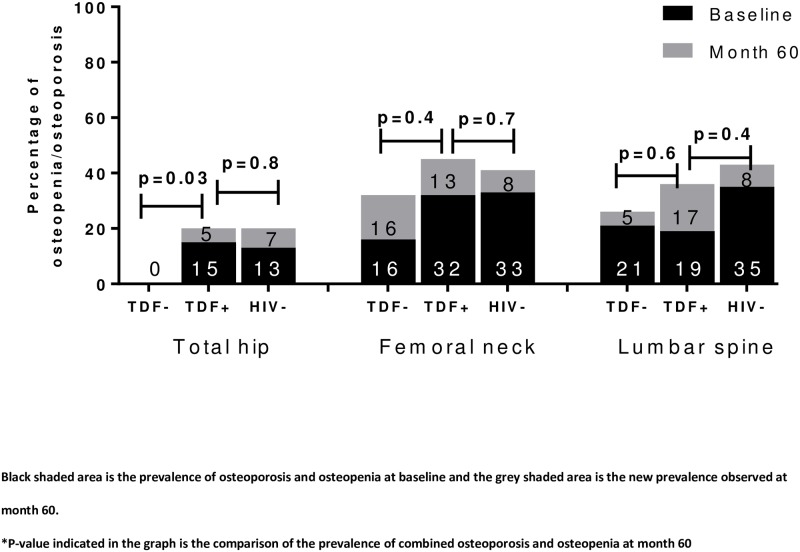
There are limited data regarding long-term BMD changes over time among treatment-naïve people living with HIV (PLHIV) after initiating combined antiretroviral therapy (cART) in Asia. We aimed to study bone mineral density (BMD) changes among treatment-naïve PLHIV started treatment with tenofovir disoproxil fumarate (TDF)- or non-TDF-containing regimen and HIV-uninfected controls in an Asian setting. The study was a five-year prospective study. BMD at lumbar spine (LS) (L1 to L4), total hip (TH), and femoral neck (FN) were measured by dual energy X-ray absorptiometry (DEXA) scans at baseline, months 12, 24 and 60. Multivariate logistic regression models were used to explore factors associated with mean BMD ≥5% reduction after 5 years of cART. A total of 106 PLHIV (75 and 31 started TDF- and non-TDF-containing regimen, respectively) and 66 HIV-uninfected individuals were enrolled. The mean percent changes of BMD were significantly different longitudinally between TDF and non-TDF users (p<0.001 for LS, p = 0.006 for TH and p = 0.02 for FN). HIV-positive status and on TDF-containing regimen was independently associated with BMD loss ≥5% at month 60 (adjusted odds ratio [aOR] 7.0, 95% confidence interval [95%CI] 2.3-21.0, P = 0.001 for LS; aOR 4.9, 95%CI 1.7-14.3, P = 0.003 for TH and aOR 4.3, 95%CI 1.6-11.2, P = 0.003 for FN) compared to HIV-uninfected individuals. In a multivariate model for PLHIV only, TDF use (vs. non-TDF, P = 0.005) and pre-treatment CD4+ count <350 cells/mm3 (vs. ≥350 cells/mm3, P = 0.02) were independently associated with ≥5% BMD loss in TH at month 60. Treatment-naïve PLHIV initiating treatment with TDF-containing regimen have higher BMD loss in a Thai cohort. TDF use and low pre-treatment CD4 count were independently associated with BMD loss at month 60 at TH. Earlier treatment initiation and interventions to prevent bone loss could improve skeletal health among PLHIV. Clinicaltrials.gov: NCT01634607.
Conflict of interest statement
KR received honoraria or consultation fees from Merck, Roche, Jensen-Cilag, Johnson & Johnson, Mylan and GPO (Governmental pharmaceutical organization, Thailand); participated in a company sponsored speaker’s bureau from Abbott, Gilead, Bristol- Myers Squibb, Merck, Roche, Jensen-Cilag, ViiV Healthcare, and GPO (Governmental pharmaceutical organization); and received Chulalongkorn Academic Advancement into Its 2nd Century Project (CUAASC). AA has received honorarium for consultation from ViiV Healthcare. We confirm that the competing interests stated do not alter our adherence to PLOS ONE policies on sharing data and materials. The rest of the authors declare no competing interests.
Figures

References
-
- Guerri-Fernandez R, Vestergaard P, Carbonell C, Knobel H, Aviles FF, Castro AS, et al. HIV infection is strongly associated with hip fracture risk, independently of age, gender, and comorbidities: a population-based cohort study. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research. 2013;28(6):1259–63. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
