

Prognostic factors for medical and productivity costs, and return to work after trauma
- PMID: 32210472
- PMCID: PMC7094860
- DOI: 10.1371/journal.pone.0230641
Prognostic factors for medical and productivity costs, and return to work after trauma
Abstract
Aim: The aim of this study was to determine prognostic factors for medical and productivity costs, and return to work (RTW) during the first two years after trauma in a clinical trauma population.
Methods: This prospective multicentre observational study followed all adult trauma patients (≥18 years) admitted to a hospital in Noord-Brabant, the Netherlands from August 2015 through November 2016. Health care consumption, productivity loss and return to work were measured in questionnaires at 1 week, 1, 3, 6, 12 and 24 months after injury. Data was linked with hospital registries. Prognostic factors for medical costs and productivity costs were analysed with log-linked gamma generalized linear models. Prognostic factors for RTW were assessed with Cox proportional hazards model. The predictive ability of the models was assessed with McFadden R2 (explained variance) and c-statistics (discrimination).
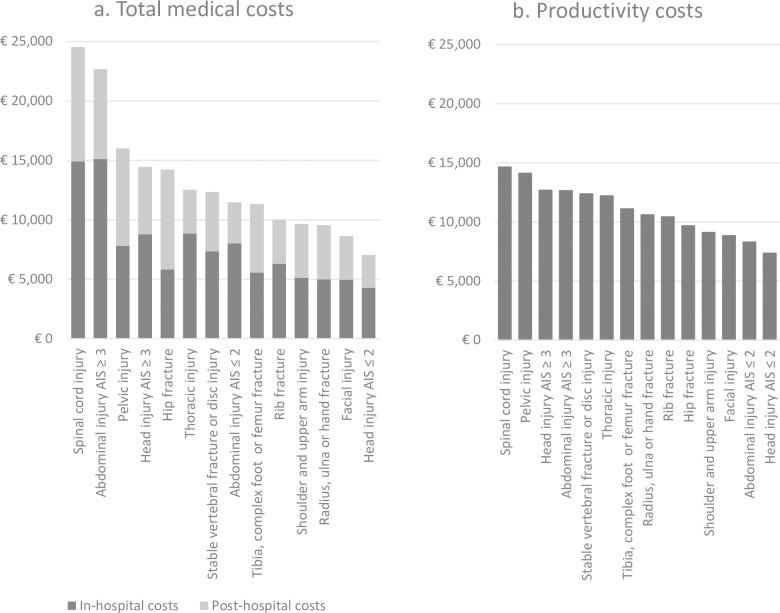
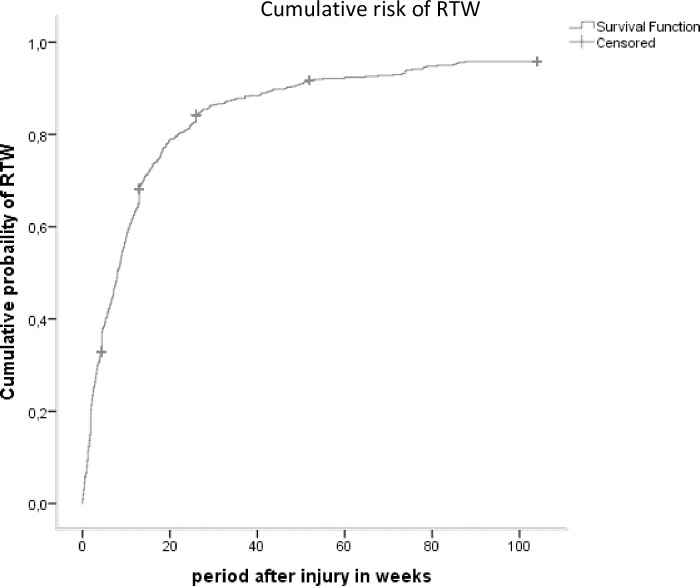
Results: A total of 3785 trauma patients (39% of total study population) responded to at least one follow-up questionnaire. Mean medical costs per patient (€9,710) and mean productivity costs per patient (€9,000) varied widely. Prognostic factors for high medical costs were higher age, female gender, spine injury, lower extremity injury, severe head injury, high injury severity, comorbidities, and pre-injury health status. Productivity costs were highest in males, and in patients with spinal cord injury, high injury severity, longer length of stay at the hospital and patients admitted to the ICU. Prognostic factors for RTW were high educational level, male gender, low injury severity, shorter length of stay at the hospital and absence of comorbidity.
Conclusions: Productivity costs and RTW should be considered when assessing the economic impact of injury in addition to medical costs. Prognostic factors may assist in identifying high cost groups with potentially modifiable factors for targeted preventive interventions, hence reducing costs and increasing RTW rates.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Landelijke Netwerk Acute Zorg (LNAZ). Annual report of the dutch trauma registry: Traumazorg in beeld 2013–2017. 2018.
-
- World Health Organization. Injuries and violence: The facts 2014. 2014;WO700(August).
-
- Xu K, Soucat A, Kutzin J, et al. Public spending on health: A closer look at global trends. 2018;WHO/HIS/HGF/HFWorkingPaper/18.3.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
