

Clinical and Immunological Outcomes in High-Risk Resected Melanoma Patients Receiving Peptide-Based Vaccination and Interferon Alpha, With or Without Dacarbazine Preconditioning: A Phase II Study
- PMID: 32211314
- PMCID: PMC7069350
- DOI: 10.3389/fonc.2020.00202
Clinical and Immunological Outcomes in High-Risk Resected Melanoma Patients Receiving Peptide-Based Vaccination and Interferon Alpha, With or Without Dacarbazine Preconditioning: A Phase II Study
Abstract
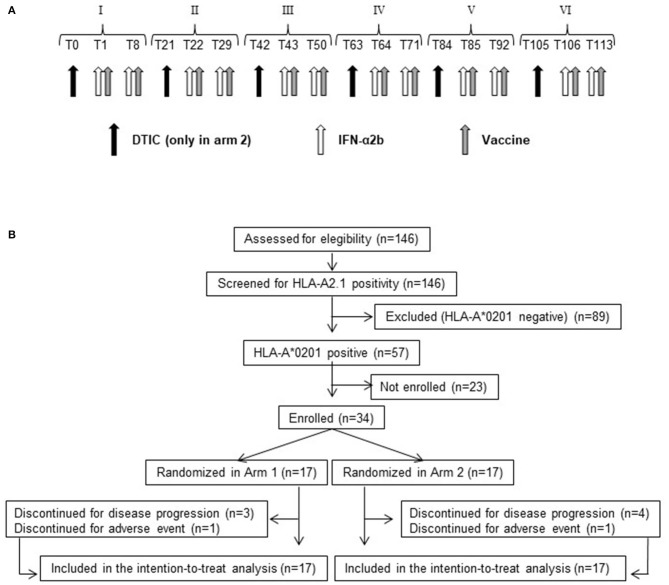
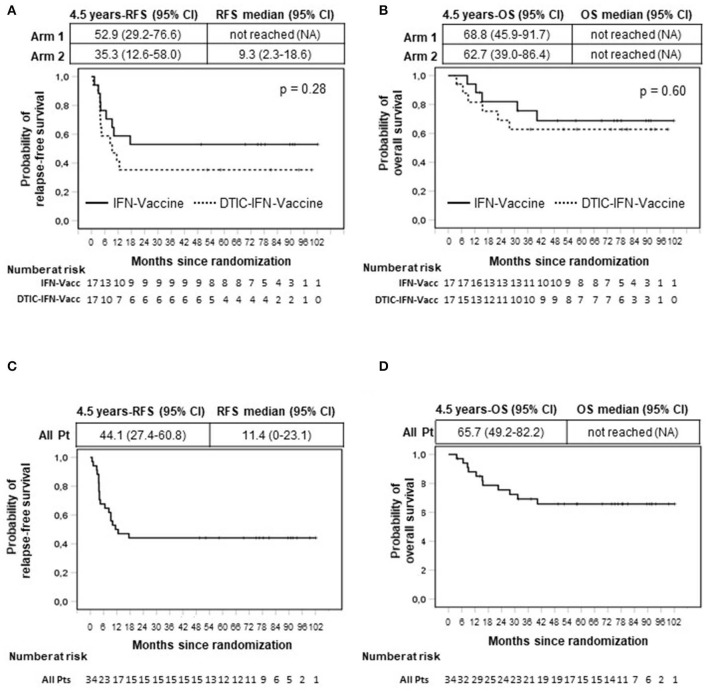
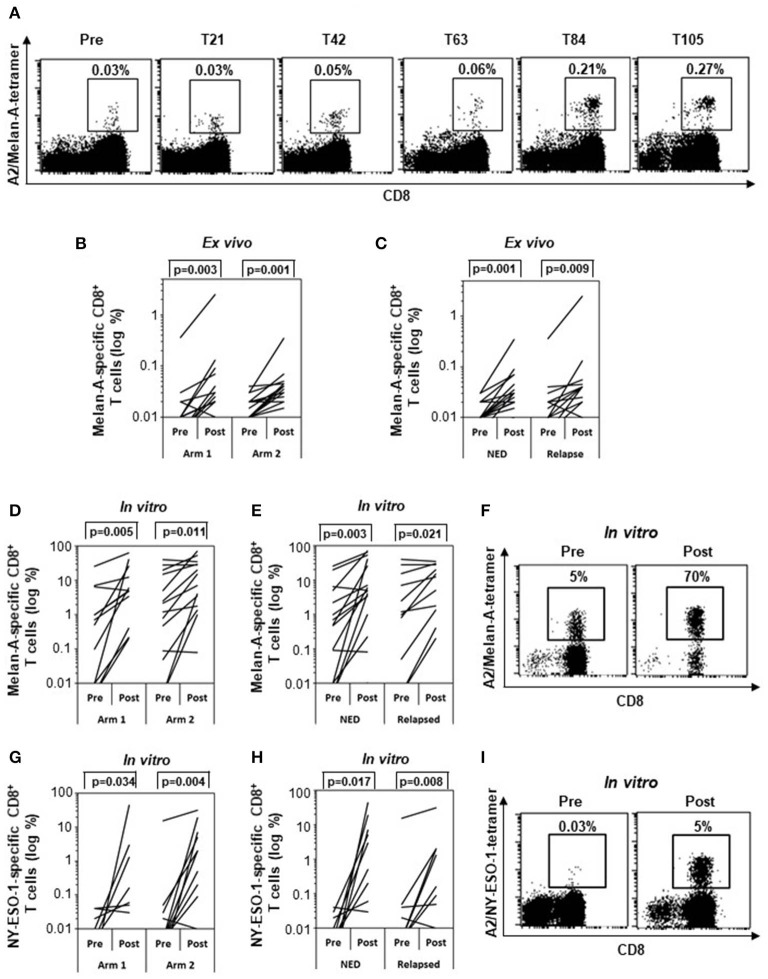
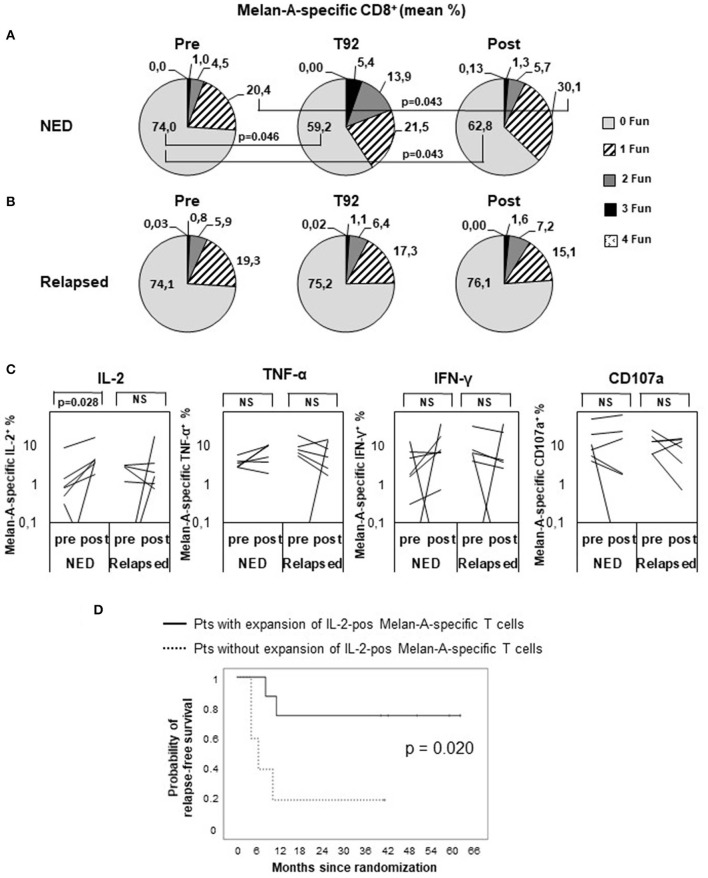
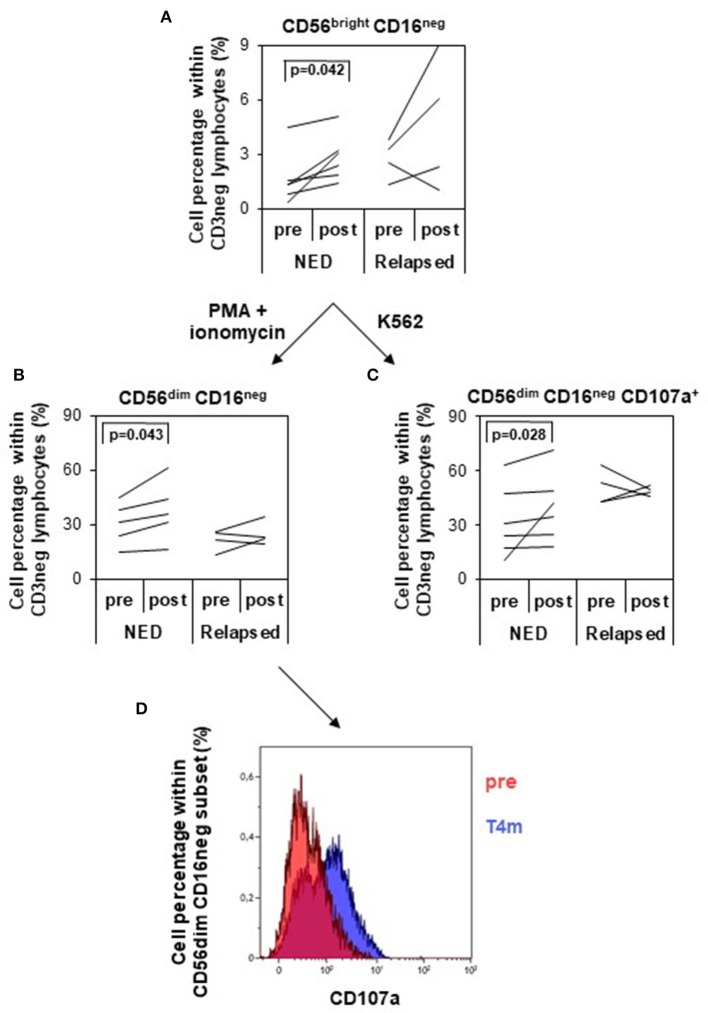
Clinical studies based on novel rationales and mechanisms of action of chemotherapy agents and cytokines can contribute to the development of new concepts and strategies of antitumor combination therapies. In previous studies, we investigated the paradoxical immunostimulating effects of some chemotherapeutics and the immunoadjuvant activity of interferon alpha (IFN-α) in preclinical and clinical models, thus unraveling novel rationales and mechanisms of action of chemotherapy agents and cytokines for cancer immunotherapy. Here, we carried out a randomized, phase II clinical trial, in which we analyzed the relapse-free (RFS) and overall survival (OS) of 34 completely resected stage III-IV melanoma patients, treated with peptide-based vaccination (Melan-A/MART-1 and NY-ESO-1) in combination with IFN-α2b, with (arm 2) or without (arm 1) dacarbazine preconditioning. All patients were included in the intention-to-treat analysis. At a median follow-up of 4.5 years (interquartile range, 15.4-81.0 months), the rates of RFS were 52.9 and 35.3% in arms 1 and 2, respectively. The 4.5-year OS rates were 68.8% in arm 1 and 62.7% in arm 2. No significant differences were observed between the two arms for both RFS and OS. Interestingly, the RFS and OS curves remained stable starting from 18 and 42 months, respectively. Grade 3 adverse events occurred in 5.9% of patients, whereas grade 4 events were not observed. Both treatments induced a significant expansion of vaccine-specific CD8+ T cells, with no correlation with the clinical outcome. However, treatment-induced increase of polyfunctionality and of interleukin 2 production by Melan-A-specific CD8+ T cells and expansion/activation of natural killer cells correlated with RFS, being observed only in nonrelapsing patients. Despite the recent availability of different therapeutic options, low-cost, low-toxic therapies with long-lasting clinical effects are still needed in patients with high-risk resected stage III/IV melanoma. The combination of peptide vaccination with IFN-α2b showed a minimal toxicity profile and resulted in encouraging RFS and OS rates, justifying further evaluation in clinical trials, which may include the use of checkpoint inhibitors to further expand the antitumor immune response and the clinical outcome. Clinical Trial Registration: https://www.clinicaltrialsregister.eu/ctr-search/search, identifier: 2008-008211-26.
Keywords: chemotherapy; combination therapy; drug repurposing; immunotherapy; interferon-α; melanoma.
Copyright © 2020 Urbani, Ferraresi, Capone, Macchia, Palermo, Nuzzo, Torsello, Pezzotti, Giannarelli, Pozzi, Santaquilani, Roazzi, Bastucci, Catricalà, La Malfa, Vercillo, Gualtieri, Buccione, Castiello, Cognetti, Nisticò, Belardelli, Moschella and Proietti.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials