

Practical considerations for performing regional anesthesia: lessons learned from the COVID-19 pandemic
- PMID: 32212103
- PMCID: PMC7095295
- DOI: 10.1007/s12630-020-01637-0
Practical considerations for performing regional anesthesia: lessons learned from the COVID-19 pandemic
Abstract
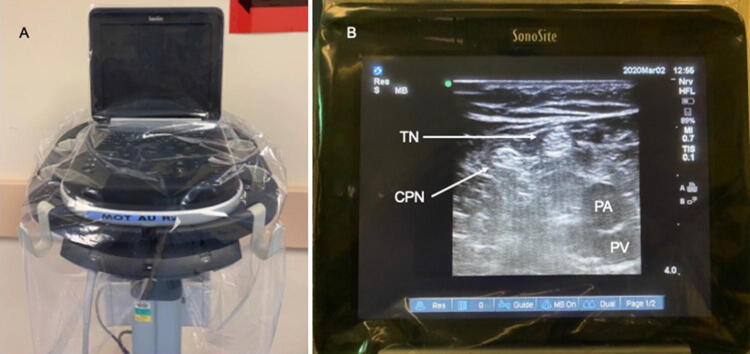
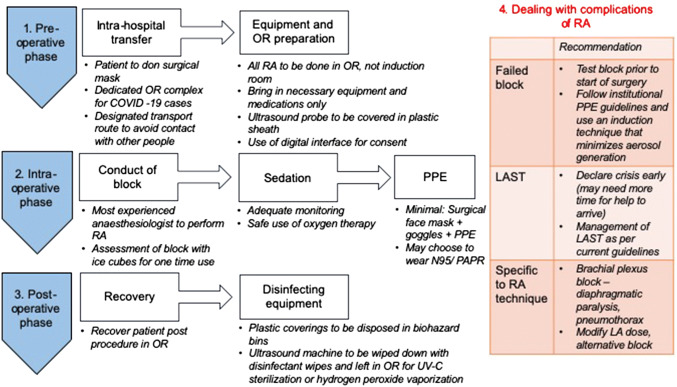
Coronavirus disease (COVID-19) was declared a pandemic by the World Health Organization on 11 March 2020 because of its rapid worldwide spread. In the operating room, as part of hospital outbreak response measures, anesthesiologists are required to have heightened precautions and tailor anesthetic practices to individual patients. In particular, by minimizing the many aerosol-generating procedures performed during general anesthesia, anesthesiologists can reduce exposure to patients' respiratory secretions and the risk of perioperative viral transmission to healthcare workers and other patients. To avoid any airway manipulation, regional anesthesia should be considered whenever surgery is planned for a suspect or confirmed COVID-19 patient or any patient who poses an infection risk. Regional anesthesia has benefits of preservation of respiratory function, avoidance of aerosolization and hence viral transmission. This article explores the practical considerations and recommended measures for performing regional anesthesia in this group of patients, focusing on control measures geared towards ensuring patient and staff safety, equipment protection, and infection prevention. By doing so, we hope to address an issue that may have downstream implications in the way we practice infection control in anesthesia, with particular relevance to this new era of emerging infectious diseases and novel pathogens. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is not the first, and certainly will not be the last novel virus that will lead to worldwide outbreaks. Having a well thought out regional anesthesia plan to manage these patients in this new normal will ensure the best possible outcome for both the patient and the perioperative management team.
RéSUMé: Le 11 mars 2020, l’Organisation mondiale de la Santé déclarait que la nouvelle maladie du coronavirus 2019 (COVID-19) était une pandémie en raison de sa propagation mondiale rapide. En salle d’opération, dans le cadre des mesures de réponse aux épidémies, les anesthésiologistes doivent prendre des précautions supplémentaires et adapter les pratiques anesthésiques au cas par cas selon chaque patient. Plus particulièrement, en minimisant les nombreuses interventions générant des aérosols pendant la réalisation de l’anesthésie générale, les anesthésiologistes peuvent réduire l’exposition aux sécrétions respiratoires des patients et le risque de transmission virale périopératoire aux travailleurs de la santé et aux autres patients. Afin d’éviter toute manipulation des voies aériennes, il convient d’envisager la réalisation d’une anesthésie régionale si une chirurgie est prévue chez un patient sous enquête de COVID-19 ou confirmé, ou chez tout patient posant un risque infectieux. L’anesthésie régionale comporte des avantages en matière de maintien de la fonction respiratoire et ce, tout en évitant la production d’aérosols et par conséquent la transmission virale. Cet article explore les considérations pratiques et les mesures recommandées pour réaliser une anesthésie régionale dans ce groupe de patients, en se concentrant sur les mesures de surveillance visant à garantir la sécurité des patients et du personnel soignant, la protection des équipements et la prévention des infections. Ce faisant, nous espérons répondre à des interrogations qui pourraient avoir des implications à plus long terme dans la manière dont nous pratiquerons la prévention de la contagion en anesthésie, avec une pertinence toute particulière pour cette nouvelle ère de maladies infectieuses émergentes et de nouveaux pathogènes. Le coronavirus du syndrome respiratoire aigu sévère 2 (SARS-CoV-2) n’est pas le premier et ne sera certainement pas le dernier nouveau virus qui entraînera des épidémies mondiales. En disposant d’un plan bien conçu d’anesthésie régionale pour prendre en charge ces patients dans cette nouvelle ère, les meilleures issues possibles seront assurées tant pour le patient que pour l’équipe de prise en charge périopératoire.
Figures


Comment in
-
Regional anesthesia during the COVID-19 pandemic: a time to reconsider practices? (Letter #1).Can J Anaesth. 2020 Sep;67(9):1282-1283. doi: 10.1007/s12630-020-01681-w. Epub 2020 May 1. Can J Anaesth. 2020. PMID: 32358763 Free PMC article. No abstract available.
-
Regional anesthesia during the COVID-19 pandemic: a time to reconsider practices? (Letter #2).Can J Anaesth. 2020 Sep;67(9):1284-1285. doi: 10.1007/s12630-020-01682-9. Epub 2020 May 1. Can J Anaesth. 2020. PMID: 32358764 Free PMC article. No abstract available.
References
-
- World Health Organization. WHO Director-General’s remarks at the media briefing on 2019-nCoV on 11 February 2020. Available from URL: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at... (accessed March 2020).
-
- World Health Organization. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Available from URL: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-... (accessed March 2020).
-
- World Health Organization. Coronavirus disease (COVID-2019) situation reports. Available from URL: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio... (accessed March 2020).
-
- World Health Organization.WHO Director-General’s opening remarks at the media briefing on COVID-19 – 11 March. Available from URL: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re... (accessed March 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
