

Efficacy and Safety of Outpatient Clinic-based Elective External Electrical Cardioversion in Patients with Atrial Fibrillation
- PMID: 32212425
- PMCID: PMC7234846
- DOI: 10.4070/kcj.2019.0310
Efficacy and Safety of Outpatient Clinic-based Elective External Electrical Cardioversion in Patients with Atrial Fibrillation
Abstract
Background and objectives: Little is known about the outcomes of outpatient clinic-based elective external cardioversion (OPC-ECV) for persistent atrial fibrillation (PeAF). We investigated the acute, short-term, and long-term elective external cardioversion (ECV) outcomes.
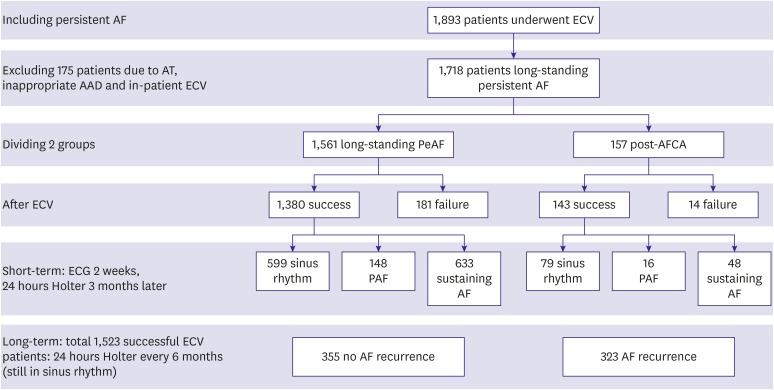
Methods: We included 1,718 patients who underwent OPC-ECV (74% male, 61.1±11.0 years old, 90.9% long-standing PeAF, 9.1% after atrial fibrillation [AF] ablation) after excluding patients with atrial tachycardia or inappropriate antiarrhythmic drug medication, and in-patient ECV. Biphasic shocks were delivered sequentially until successful cardioversion was achieved (70-100-150-200-250 J). If ECV failed at 150 J, we administered intravenous amiodarone 150 mg and delivered 200 J.
Results: ECV failed in 11.4%, and the complication rate was 0.47%. Within 3 months, AF recurred in 55.5% (44.7% as sustaining AF, 10.8% as paroxysmal AF), and the AF duration was independently associated (odds ratio [OR], 1.01 [1.00-1.02]; p=0.006), but amiodarone was independently protective (OR, 0.46 [0.27-0.76]; p=0.002, Log rank p<0.001) against an early recurrence. Regarding the long-term recurrence, pre-ECV heart failure was protective against an AF recurrence (hazard ratio, 0.63 [0.41-0.96], p=0.033) over 32 (9-66) months of follow-up. ECV energy (p<0.001) and early recurrence rate within 3 months (p=0.007, Log rank p=0.006) were significantly lower in post-ablation patients than in those with long-standing persistent AF.
Conclusions: The success rate of OPC-ECV was 88.6%, and the complication rate was low. However, AF recurred in 55.5% within 3 months. Amiodarone was protective against short-term AF recurrences, and long-term AF recurrences were less in patients with baseline heart failure.
Keywords: Atrial fibrillation; Cardioversion; Recurrence.
Copyright © 2020. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

References
-
- Kim D, Yang PS, Jang E, et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. 2018;202:20–26. - PubMed
-
- Marrouche NF, Brachmann J, Andresen D, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378:417–427. - PubMed
-
- Mansour M, Heist EK, Agarwal R, et al. Stroke and cardiovascular events after ablation or antiarrhythmic drugs for treatment of patients with atrial fibrillation. Am J Cardiol. 2018;121:1192–1199. - PubMed
-
- Jin MN, Kim TH, Kang KW, et al. Atrial fibrillation catheter ablation improves 1-year follow-up cognitive function, especially in patients with impaired cognitive function. Circ Arrhythm Electrophysiol. 2019;12:e007197. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
