

Clinical Potential of Targeting Fibroblast Growth Factor-23 and αKlotho in the Treatment of Uremic Cardiomyopathy
- PMID: 32212912
- PMCID: PMC7428638
- DOI: 10.1161/JAHA.120.016041
Clinical Potential of Targeting Fibroblast Growth Factor-23 and αKlotho in the Treatment of Uremic Cardiomyopathy
Erratum in
-
Correction to: Clinical Potential of Targeting Fibroblast Growth Factor-23 and αKlotho in the Treatment of Uremic Cardiomyopathy.J Am Heart Assoc. 2020 Jul 21;9(14):e014566. doi: 10.1161/JAHA.119.014566. Epub 2020 Jul 17. J Am Heart Assoc. 2020. PMID: 32674722 Free PMC article. No abstract available.
Abstract
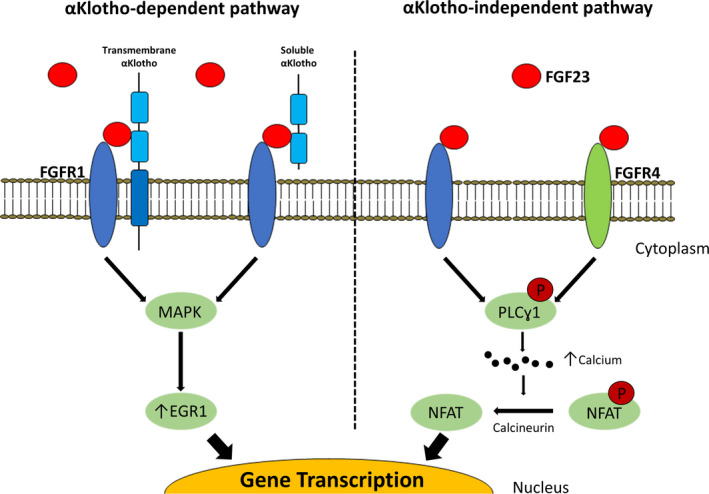
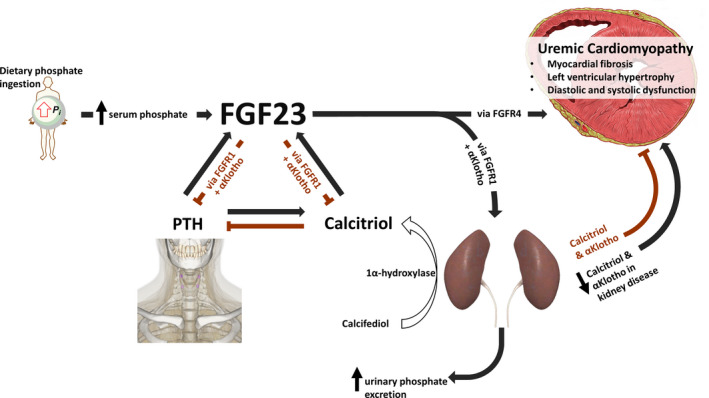
Chronic kidney disease is highly prevalent, affecting 10% to 15% of the adult population worldwide and is associated with increased cardiovascular morbidity and mortality. As chronic kidney disease worsens, a unique cardiovascular phenotype develops characterized by heart muscle disease, increased arterial stiffness, atherosclerosis, and hypertension. Cardiovascular risk is multifaceted, but most cardiovascular deaths in patients with advanced chronic kidney disease are caused by heart failure and sudden cardiac death. While the exact drivers of these deaths are unknown, they are believed to be caused by uremic cardiomyopathy: a specific pattern of myocardial hypertrophy, fibrosis, with both diastolic and systolic dysfunction. Although the pathogenesis of uremic cardiomyopathy is likely to be multifactorial, accumulating evidence suggests increased production of fibroblast growth factor-23 and αKlotho deficiency as potential major drivers of cardiac remodeling in patients with uremic cardiomyopathy. In this article we review the increasing understanding of the physiology and clinical aspects of uremic cardiomyopathy and the rapidly increasing knowledge of the biology of both fibroblast growth factor-23 and αKlotho. Finally, we discuss how dissection of these pathological processes is aiding the development of therapeutic options, including small molecules and antibodies, directly aimed at improving the cardiovascular outcomes of patients with chronic kidney disease and end-stage renal disease.
Keywords: FGF23; cardiorenal syndrome; fibroblast growth factor; growth factor; kidney; treatment; αKlotho.
Figures
Similar articles
-
New Insights into the Role of FGF-23 and Klotho in Cardiovascular Disease in Chronic Kidney Disease Patients.Curr Vasc Pharmacol. 2021;19(1):55-62. doi: 10.2174/1570161118666200420102100. Curr Vasc Pharmacol. 2021. PMID: 32310050 Review.
-
αKlotho attenuates cardiac hypertrophy and increases myocardial fibroblast growth factor 21 expression in uremic rats.Exp Biol Med (Maywood). 2020 Jan;245(1):66-78. doi: 10.1177/1535370219894302. Epub 2019 Dec 17. Exp Biol Med (Maywood). 2020. PMID: 31847589 Free PMC article.
-
Soluble Klotho Protects against Uremic Cardiomyopathy Independently of Fibroblast Growth Factor 23 and Phosphate.J Am Soc Nephrol. 2015 May;26(5):1150-60. doi: 10.1681/ASN.2014040325. Epub 2014 Dec 4. J Am Soc Nephrol. 2015. PMID: 25475745 Free PMC article.
-
αKlotho and Chronic Kidney Disease.Vitam Horm. 2016;101:257-310. doi: 10.1016/bs.vh.2016.02.007. Epub 2016 Mar 24. Vitam Horm. 2016. PMID: 27125746 Free PMC article. Review.
-
Cardioprotective Effects of Paricalcitol Alone and in Combination With FGF23 Receptor Inhibition in Chronic Renal Failure: Experimental and Clinical Studies.Am J Hypertens. 2019 Jan 1;32(1):34-44. doi: 10.1093/ajh/hpy154. Am J Hypertens. 2019. PMID: 30329020 Free PMC article.
Cited by
-
Risk for subsequent hypertension and cardiovascular disease after living kidney donation: is it clinically relevant?Clin Kidney J. 2021 Dec 13;15(4):644-656. doi: 10.1093/ckj/sfab271. eCollection 2022 Apr. Clin Kidney J. 2021. PMID: 35371443 Free PMC article. Review.
-
An angiopoietin 2, FGF23, and BMP10 biomarker signature differentiates atrial fibrillation from other concomitant cardiovascular conditions.Sci Rep. 2023 Oct 5;13(1):16743. doi: 10.1038/s41598-023-42331-7. Sci Rep. 2023. PMID: 37798357 Free PMC article.
-
Baseline fibroblast growth factor 23 predicts incident heart failure and cardiovascular mortality in patients with chronic kidney disease: A 3-year follow-up study.Int J Cardiol Heart Vasc. 2024 Dec 23;56:101587. doi: 10.1016/j.ijcha.2024.101587. eCollection 2025 Feb. Int J Cardiol Heart Vasc. 2024. PMID: 39807363 Free PMC article.
-
Clinical impact of diastolic dysfunction and atrial fibrillation before and after initiating hemodialysis in patients with end-stage kidney disease.Ren Fail. 2024 Dec;46(2):2401623. doi: 10.1080/0886022X.2024.2401623. Epub 2024 Sep 23. Ren Fail. 2024. PMID: 39313766 Free PMC article.
-
Neutrophil extracellular traps aggravate uremic cardiomyopathy by inducing myocardial fibroblast pyroptosis.Sci Rep. 2025 May 20;15(1):17509. doi: 10.1038/s41598-025-02383-3. Sci Rep. 2025. PMID: 40394287 Free PMC article.
References
-
- Levin A, Tonelli M, Bonventre J, Coresh J, Donner JA, Fogo AB, Fox CS, Gansevoort RT, Heerspink HJL, Jardine M, et al. Global kidney health 2017 and beyond: a roadmap for closing gaps in care, research, and policy. Lancet. 2017;390:1888–1917. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Chronic Kidney Disease Prognosis C , Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all‐cause and cardiovascular mortality in general population cohorts: a collaborative meta‐analysis. Lancet. 2010;375:2073–2081. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
