

Natural history, diagnosis and treatment approach to fibrostenosing Crohn's disease
- PMID: 32213020
- PMCID: PMC7184664
- DOI: 10.1177/2050640620901960
Natural history, diagnosis and treatment approach to fibrostenosing Crohn's disease
Abstract
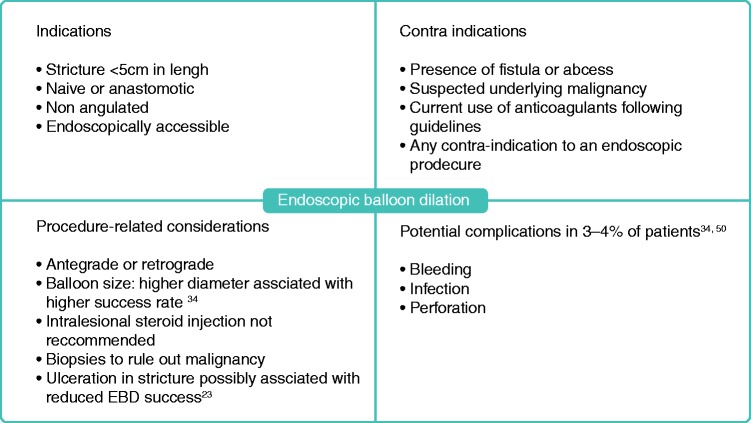
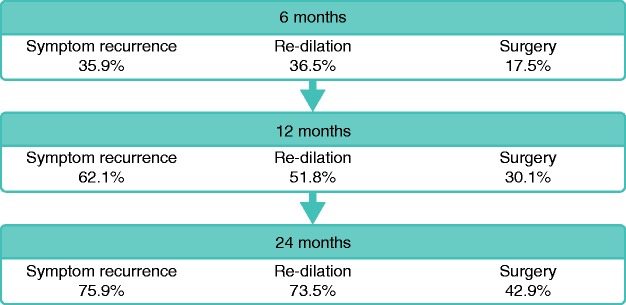
Stricturing Crohn's disease (CD) is a significant clinical problem. The presence of a stricture may be suggested by clinical symptoms. Cross-sectional imaging using computed tomography or magnetic resonance enterography is essential in diagnosing strictures as it allows further characterization and evaluation for complications such as abscess, fistulizing disease or malignancy. Managing small bowel stricturing CD should be approached in a multidisciplinary fashion. Medical therapy can be considered in strictures which are not associated with complications, with most of the data supporting anti-TNF strategies in this setting. If the disease is refractory to medical therapy, endoscopic therapy or surgery should be performed. Endoscopic balloon dilation (EBD) is an option for short, uncomplicated and straight strictures that are within reach of a colonoscope. Although EBD has good short-term outcomes, repeat dilation is often required. Surgical options mainly include resection and strictureplasty. Strictures refractory to medical therapy, not amenable or refractory to EBD, or associated with complications or malignancy should be managed surgically. However, surgery may also be considered at an earlier stage depending on disease characteristics and patient preference. Postoperative recurrence is common, highlighting the importance of careful monitoring of the patient postoperatively and optimization of medical management accordingly. There is a pressing need to develop anti-fibrotics for the treatment of stricturing CD. This requires the development of standardized diagnostic criteria, patient-reported outcome measures and validation of endpoints in fibrostenotic CD. The STAR consortium is pioneering this effort in order to allow development and testing of anti-fibrotics in future clinical trials.
Keywords: Crohn’s disease; Stricture; endoscopic balloon dilation; fibrosis; inflammatory bowel disease; stenosis; surgery.
Figures
References
-
- Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990; 99: 956–963. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
