Pancreatic cancer-derived organoids - a disease modeling tool to predict drug response
- PMID: 32213029
- PMCID: PMC7268941
- DOI: 10.1177/2050640620905183
Pancreatic cancer-derived organoids - a disease modeling tool to predict drug response
Erratum in
-
Corrigendum.United European Gastroenterol J. 2020 Oct;8(8):987. doi: 10.1177/2050640620944750. United European Gastroenterol J. 2020. PMID: 32981490 Free PMC article. No abstract available.
Abstract
Background: Organotypic cultures derived from pancreatic ductal adenocarcinoma (PDAC) termed pancreatic ductal cancer organoids (PDOs) recapitulate the primary cancer and can be derived from primary or metastatic biopsies. Although isolation and culture of patient-derived pancreatic organoids were established several years ago, pros and cons for individualized medicine have not been comprehensively investigated to date.
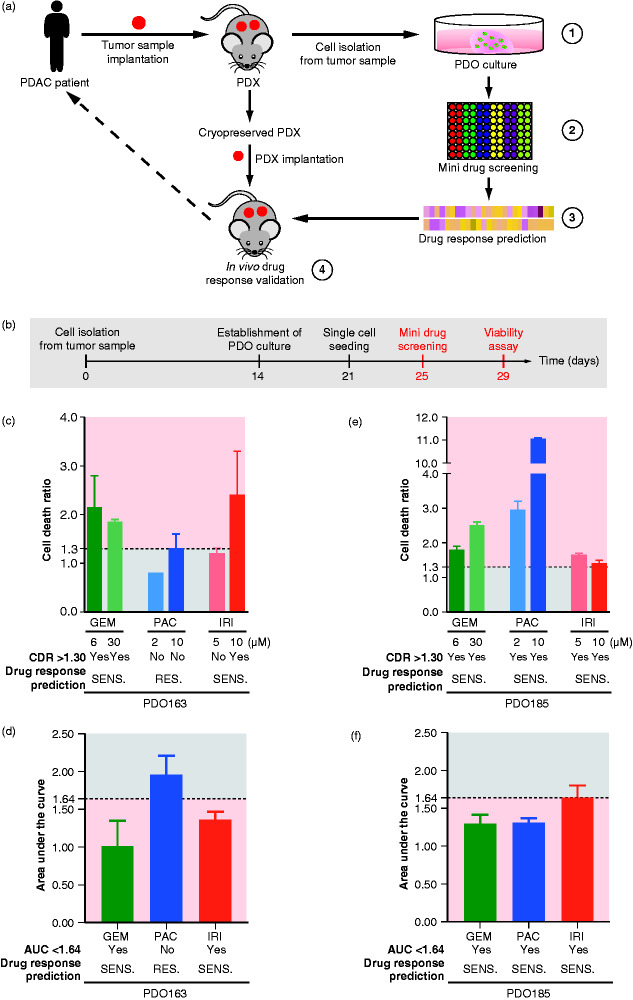
Methods: We conducted a feasibility study, systematically comparing head-to-head patient-derived xenograft tumor (PDX) and PDX-derived organoids by rigorous immunohistochemical and molecular characterization. Subsequently, a drug testing platform was set up and validated in vivo. Patient-derived organoids were investigated as well.
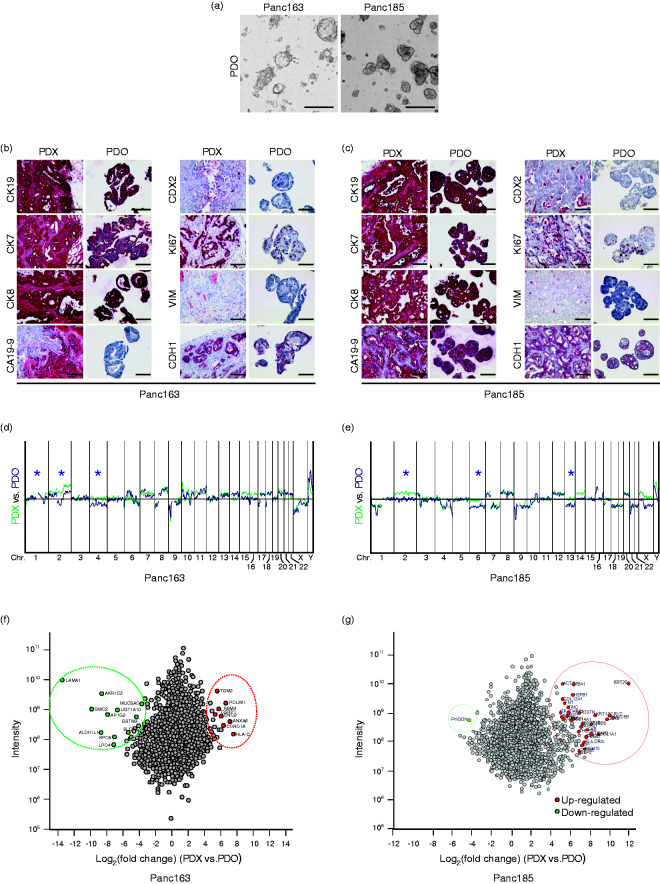
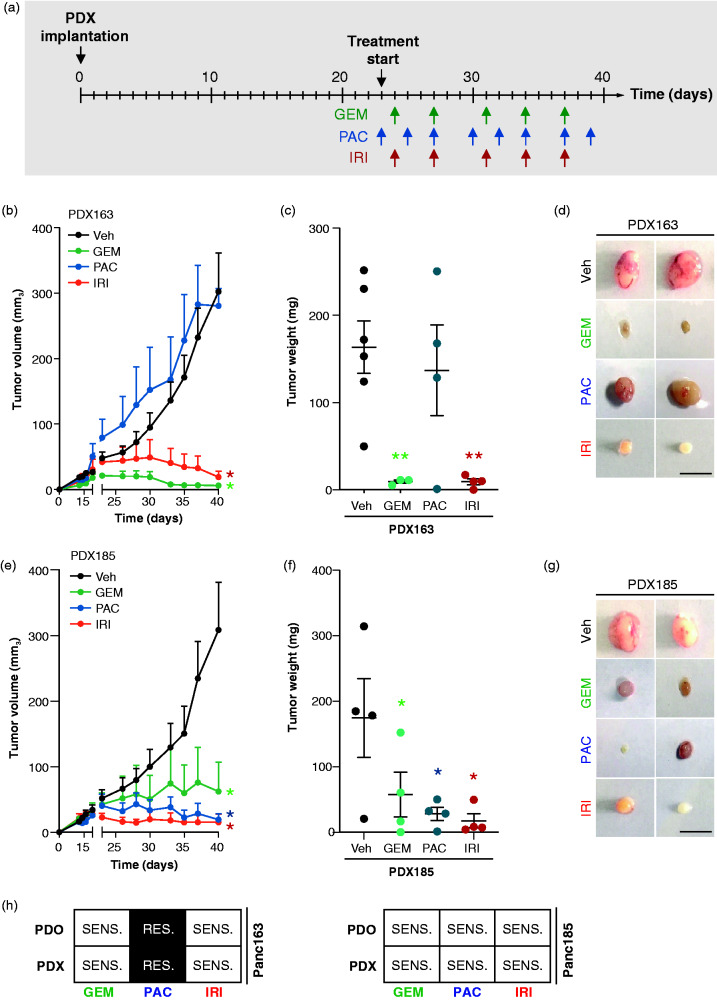
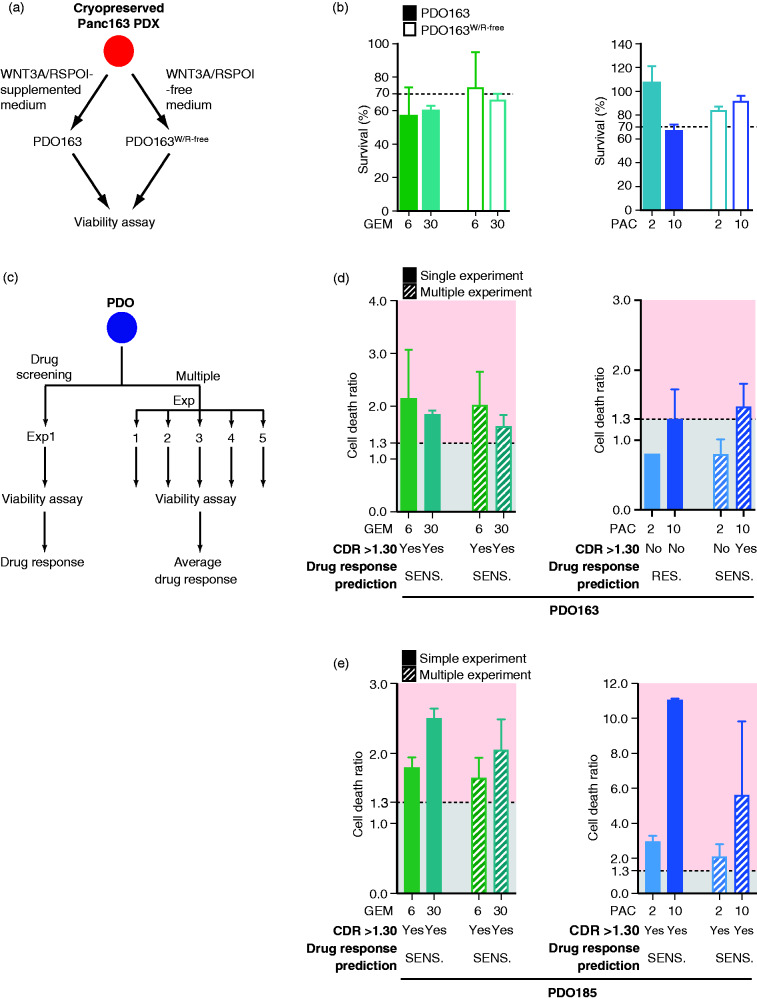
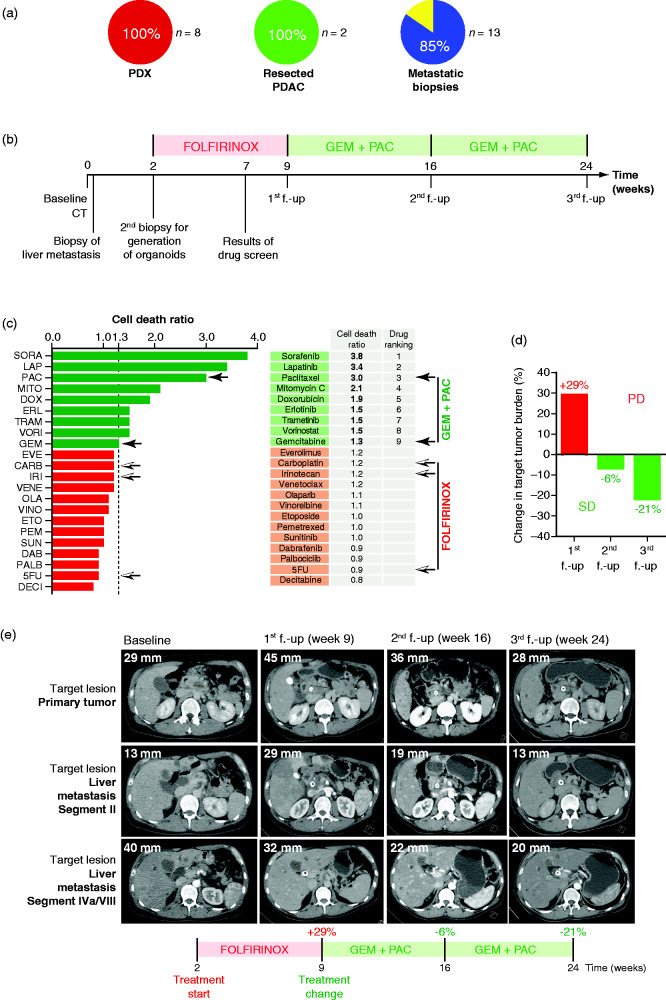
Results: First, PDOs faithfully recapitulated the morphology and marker protein expression patterns of the PDXs. Second, quantitative proteomes from the PDX as well as from corresponding organoid cultures showed high concordance. Third, genomic alterations, as assessed by array-based comparative genomic hybridization, revealed similar results in both groups. Fourth, we established a small-scale pharmacotyping platform adjusted to operate in parallel considering potential obstacles such as culture conditions, timing, drug dosing, and interpretation of the results. In vitro predictions were successfully validated in an in vivo xenograft trial. Translational proof-of-concept is exemplified in a patient with PDAC receiving palliative chemotherapy.
Conclusion: Small-scale drug screening in organoids appears to be a feasible, robust and easy-to-handle disease modeling method to allow response predictions in parallel to daily clinical routine. Therefore, our fast and cost-efficient assay is a reasonable approach in a predictive clinical setting.
Keywords: PDAC; drug response prediction; organoids.
Figures