

Interventions to mitigate early spread of SARS-CoV-2 in Singapore: a modelling study
- PMID: 32213332
- PMCID: PMC7158571
- DOI: 10.1016/S1473-3099(20)30162-6
Interventions to mitigate early spread of SARS-CoV-2 in Singapore: a modelling study
Erratum in
-
Correction to Lancet Infect Dis 2020; published online March 23. https://doi.org/10.1016/S1473-3099(20)30162.Lancet Infect Dis. 2020 May;20(5):e79. doi: 10.1016/S1473-3099(20)30261-9. Epub 2020 Mar 27. Lancet Infect Dis. 2020. PMID: 32224309 Free PMC article. No abstract available.
Abstract
Background: Since the coronavirus disease 2019 outbreak began in the Chinese city of Wuhan on Dec 31, 2019, 68 imported cases and 175 locally acquired infections have been reported in Singapore. We aimed to investigate options for early intervention in Singapore should local containment (eg, preventing disease spread through contact tracing efforts) be unsuccessful.
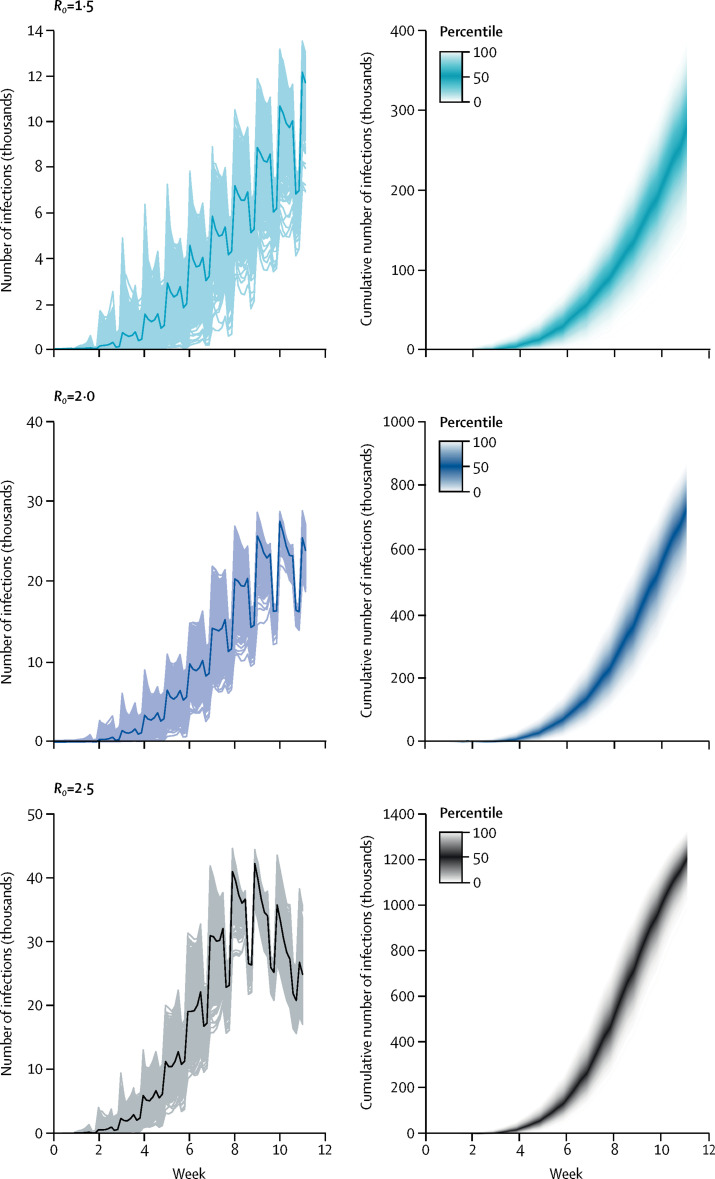
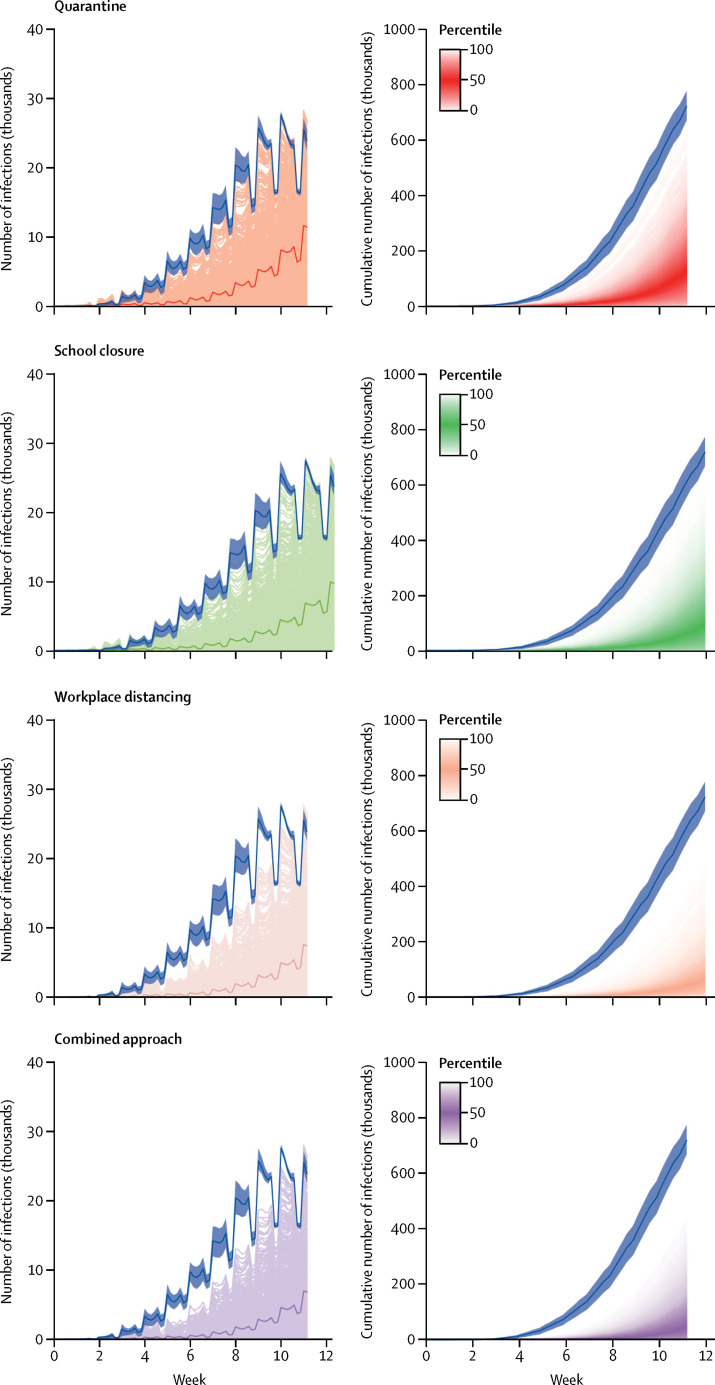
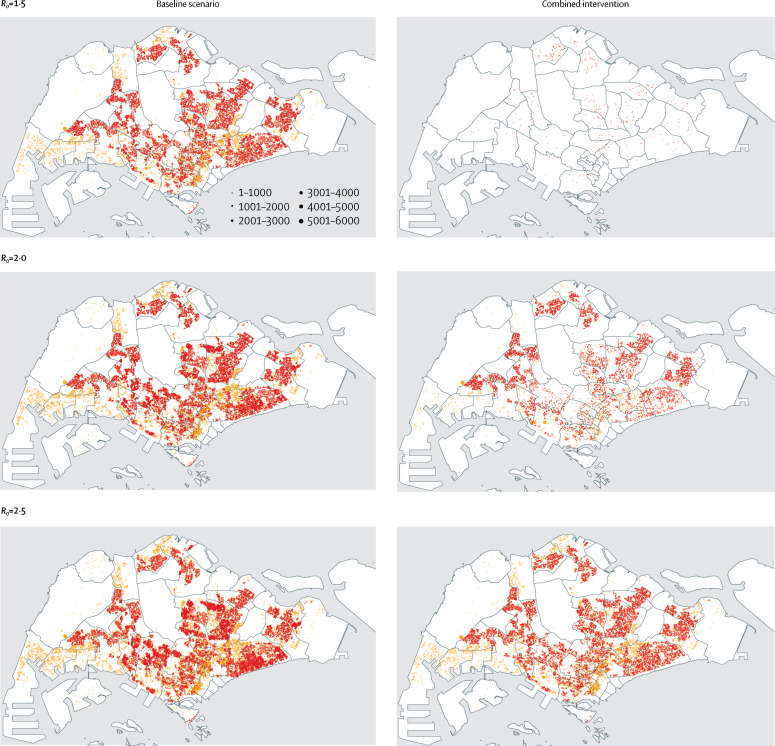
Methods: We adapted an influenza epidemic simulation model to estimate the likelihood of human-to-human transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a simulated Singaporean population. Using this model, we estimated the cumulative number of SARS-CoV-2 infections at 80 days, after detection of 100 cases of community transmission, under three infectivity scenarios (basic reproduction number [R0] of 1·5, 2·0, or 2·5) and assuming 7·5% of infections are asymptomatic. We first ran the model assuming no intervention was in place (baseline scenario), and then assessed the effect of four intervention scenarios compared with a baseline scenario on the size and progression of the outbreak for each R0 value. These scenarios included isolation measures for infected individuals and quarantining of family members (hereafter referred to as quarantine); quarantine plus school closure; quarantine plus workplace distancing; and quarantine, school closure, and workplace distancing (hereafter referred to as the combined intervention). We also did sensitivity analyses by altering the asymptomatic fraction of infections (22·7%, 30·0%, 40·0%, and 50·0%) to compare outbreak sizes under the same control measures.
Findings: For the baseline scenario, when R0 was 1·5, the median cumulative number of infections at day 80 was 279 000 (IQR 245 000-320 000), corresponding to 7·4% (IQR 6·5-8·5) of the resident population of Singapore. The median number of infections increased with higher infectivity: 727 000 cases (670 000-776 000) when R0 was 2·0, corresponding to 19·3% (17·8-20·6) of the Singaporean population, and 1 207 000 cases (1 164 000-1 249 000) when R0 was 2·5, corresponding to 32% (30·9-33·1) of the Singaporean population. Compared with the baseline scenario, the combined intervention was the most effective, reducing the estimated median number of infections by 99·3% (IQR 92·6-99·9) when R0 was 1·5, by 93·0% (81·5-99·7) when R0 was 2·0, and by 78·2% (59·0 -94·4) when R0 was 2·5. Assuming increasing asymptomatic fractions up to 50·0%, up to 277 000 infections were estimated to occur at day 80 with the combined intervention relative to 1800 for the baseline at R0 of 1·5.
Interpretation: Implementing the combined intervention of quarantining infected individuals and their family members, workplace distancing, and school closure once community transmission has been detected could substantially reduce the number of SARS-CoV-2 infections. We therefore recommend immediate deployment of this strategy if local secondary transmission is confirmed within Singapore. However, quarantine and workplace distancing should be prioritised over school closure because at this early stage, symptomatic children have higher withdrawal rates from school than do symptomatic adults from work. At higher asymptomatic proportions, intervention effectiveness might be substantially reduced requiring the need for effective case management and treatments, and preventive measures such as vaccines.
Funding: Singapore Ministry of Health, Singapore Population Health Improvement Centre.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Scientific and ethical basis for social-distancing interventions against COVID-19.Lancet Infect Dis. 2020 Jun;20(6):631-633. doi: 10.1016/S1473-3099(20)30190-0. Epub 2020 Mar 23. Lancet Infect Dis. 2020. PMID: 32213329 Free PMC article. No abstract available.
References
-
- WHO Pneumonia of unknown cause–China. Jan 5, 2020. https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-ch...
-
- WHO Novel coronavirus (2019-nCoV) situation report–3. Jan 23, 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
