

Artificial intelligence versus clinicians: systematic review of design, reporting standards, and claims of deep learning studies
- PMID: 32213531
- PMCID: PMC7190037
- DOI: 10.1136/bmj.m689
Artificial intelligence versus clinicians: systematic review of design, reporting standards, and claims of deep learning studies
Abstract
Objective: To systematically examine the design, reporting standards, risk of bias, and claims of studies comparing the performance of diagnostic deep learning algorithms for medical imaging with that of expert clinicians.
Design: Systematic review.
Data sources: Medline, Embase, Cochrane Central Register of Controlled Trials, and the World Health Organization trial registry from 2010 to June 2019.
Eligibility criteria for selecting studies: Randomised trial registrations and non-randomised studies comparing the performance of a deep learning algorithm in medical imaging with a contemporary group of one or more expert clinicians. Medical imaging has seen a growing interest in deep learning research. The main distinguishing feature of convolutional neural networks (CNNs) in deep learning is that when CNNs are fed with raw data, they develop their own representations needed for pattern recognition. The algorithm learns for itself the features of an image that are important for classification rather than being told by humans which features to use. The selected studies aimed to use medical imaging for predicting absolute risk of existing disease or classification into diagnostic groups (eg, disease or non-disease). For example, raw chest radiographs tagged with a label such as pneumothorax or no pneumothorax and the CNN learning which pixel patterns suggest pneumothorax.
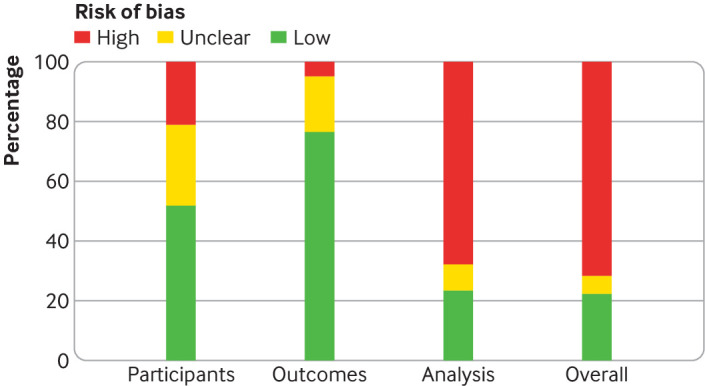
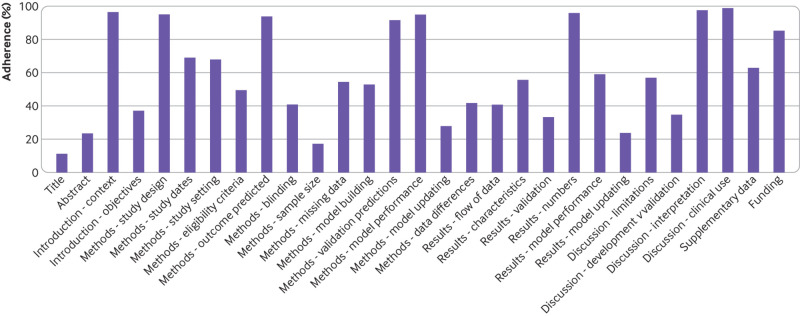
Review methods: Adherence to reporting standards was assessed by using CONSORT (consolidated standards of reporting trials) for randomised studies and TRIPOD (transparent reporting of a multivariable prediction model for individual prognosis or diagnosis) for non-randomised studies. Risk of bias was assessed by using the Cochrane risk of bias tool for randomised studies and PROBAST (prediction model risk of bias assessment tool) for non-randomised studies.
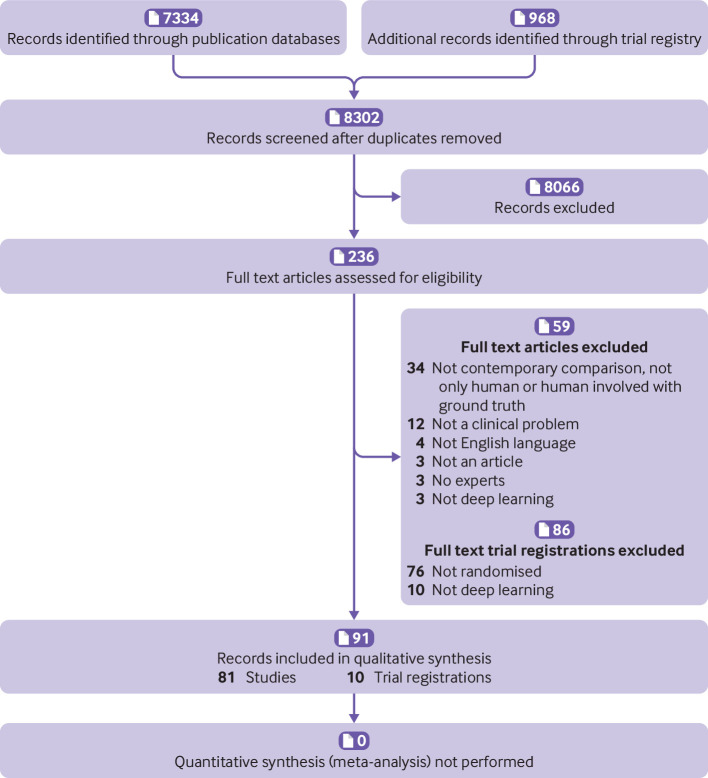
Results: Only 10 records were found for deep learning randomised clinical trials, two of which have been published (with low risk of bias, except for lack of blinding, and high adherence to reporting standards) and eight are ongoing. Of 81 non-randomised clinical trials identified, only nine were prospective and just six were tested in a real world clinical setting. The median number of experts in the comparator group was only four (interquartile range 2-9). Full access to all datasets and code was severely limited (unavailable in 95% and 93% of studies, respectively). The overall risk of bias was high in 58 of 81 studies and adherence to reporting standards was suboptimal (<50% adherence for 12 of 29 TRIPOD items). 61 of 81 studies stated in their abstract that performance of artificial intelligence was at least comparable to (or better than) that of clinicians. Only 31 of 81 studies (38%) stated that further prospective studies or trials were required.
Conclusions: Few prospective deep learning studies and randomised trials exist in medical imaging. Most non-randomised trials are not prospective, are at high risk of bias, and deviate from existing reporting standards. Data and code availability are lacking in most studies, and human comparator groups are often small. Future studies should diminish risk of bias, enhance real world clinical relevance, improve reporting and transparency, and appropriately temper conclusions.
Study registration: PROSPERO CRD42019123605.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; CAL worked as clinical data science and technology lead for Cera, a technology enabled homecare provider; ACG reports that outside of this work he has received speaker fees from Orion Corporation Orion Pharma and Amomed Pharma, has consulted for Ferring Pharmaceuticals, Tenax Therapeutics, Baxter Healthcare, Bristol-Myers Squibb and GSK, and received grant support from Orion Corporation Orion Pharma, Tenax Therapeutics, and HCA International with funds paid to his institution; HH was previously clinical director of Kheiron Medical Technologies and is now director at Hardian Health; EJT is on the scientific advisory board of Verily, Tempus Laboratories, Myokardia, and Voxel Cloud, the board of directors of Dexcoman, and is an advisor to Guardant Health, Blue Cross Blue Shield Association, and Walgreens; MM is a cofounder of Cera, a technology enabled homecare provider, board member of the NHS Innovation Accelerator, and senior advisor to Bain and Co.
Figures
Comment in
-
Artificial intelligence versus clinicians.BMJ. 2020 Apr 3;369:m1326. doi: 10.1136/bmj.m1326. BMJ. 2020. PMID: 32245846 No abstract available.
-
Postgraduate medical education after COVID-19: reflections on decision-making and the state of UK medical Grand Rounds.Postgrad Med J. 2022 Mar;98(e2):e94-e95. doi: 10.1136/postgradmedj-2020-139032. Postgrad Med J. 2022. PMID: 35232850 No abstract available.
References
-
- Carson E. IBM Watson Health computes a pair of new solutions to improve healthcare data and security. 2015. https://www.techrepublic.com/article/ibm-watson-health-computes-a-pair-o....
-
- ReportLinker. Artificial intelligence in healthcare market by offering, technology, end-use application, end user and geography – global forecast to 2025. 2018. https://www.reportlinker.com/p04897122/Artificial-Intelligence-in-Health....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical