

Current Landscape and Emerging Fields of PET Imaging in Patients with Brain Tumors
- PMID: 32213992
- PMCID: PMC7146177
- DOI: 10.3390/molecules25061471
Current Landscape and Emerging Fields of PET Imaging in Patients with Brain Tumors
Abstract
The number of positron-emission tomography (PET) tracers used to evaluate patients with brain tumors has increased substantially over the last years. For the management of patients with brain tumors, the most important indications are the delineation of tumor extent (e.g., for planning of resection or radiotherapy), the assessment of treatment response to systemic treatment options such as alkylating chemotherapy, and the differentiation of treatment-related changes (e.g., pseudoprogression or radiation necrosis) from tumor progression. Furthermore, newer PET imaging approaches aim to address the need for noninvasive assessment of tumoral immune cell infiltration and response to immunotherapies (e.g., T-cell imaging). This review summarizes the clinical value of the landscape of tracers that have been used in recent years for the above-mentioned indications and also provides an overview of promising newer tracers for this group of patients.
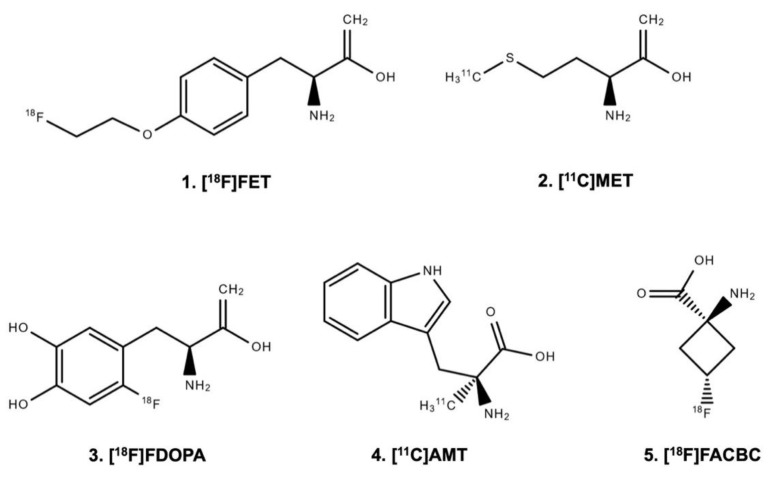
Keywords: FACBC; FDOPA; FET; amino acid; brain metastases; glioma; immunoPET; molecular imaging.
Conflict of interest statement
Related to the present work, the authors disclosed no potential conflicts of interest.
Figures
References
-
- Lohmann P., Stavrinou P., Lipke K., Bauer E.K., Ceccon G., Werner J.M., Neumaier B., Fink G.R., Shah N.J., Langen K.J., et al. FET PET reveals considerable spatial differences in tumour burden compared to conventional MRI in newly diagnosed glioblastoma. Eur. J. Nucl. Med. Mol. Imaging. 2019;46:591–602. doi: 10.1007/s00259-018-4188-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
