

Influenza Vaccine Effectiveness by A(H3N2) Phylogenetic Subcluster and Prior Vaccination History: 2016-2017 and 2017-2018 Epidemics in Canada
- PMID: 32215564
- PMCID: PMC9016427
- DOI: 10.1093/infdis/jiaa138
Influenza Vaccine Effectiveness by A(H3N2) Phylogenetic Subcluster and Prior Vaccination History: 2016-2017 and 2017-2018 Epidemics in Canada
Abstract
Background: The influenza A(H3N2) vaccine was updated from clade 3C.3a in 2015-2016 to 3C.2a for 2016-2017 and 2017-2018. Circulating 3C.2a viruses showed considerable hemagglutinin glycoprotein diversification and the egg-adapted vaccine also bore mutations.
Methods: Vaccine effectiveness (VE) in 2016-2017 and 2017-2018 was assessed by test-negative design, explored by A(H3N2) phylogenetic subcluster and prior season's vaccination history.
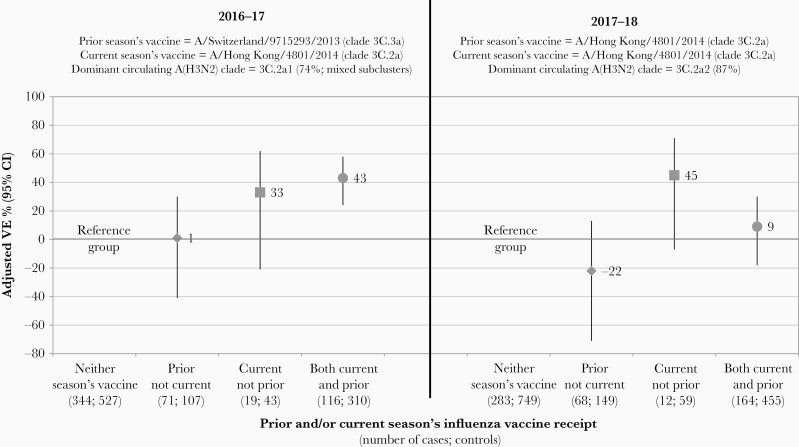
Results: In 2016-2017, A(H3N2) VE was 36% (95% confidence interval [CI], 18%-50%), comparable with (43%; 95% CI, 24%-58%) or without (33%; 95% CI, -21% to 62%) prior season's vaccination. In 2017-2018, VE was 14% (95% CI, -8% to 31%), lower with (9%; 95% CI, -18% to 30%) versus without (45%; 95% CI, -7% to 71%) prior season's vaccination. In 2016-2017, VE against predominant clade 3C.2a1 viruses was 33% (95% CI, 11%-50%): 18% (95% CI, -40% to 52%) for 3C.2a1a defined by a pivotal T135K loss of glycosylation; 60% (95% CI, 19%-81%) for 3C.2a1b (without T135K); and 31% (95% CI, 2%-51%) for other 3C.2a1 variants (with/without T135K). VE against 3C.2a2 viruses was 45% (95% CI, 2%-70%) in 2016-2017 but 15% (95% CI, -7% to 33%) in 2017-2018 when 3C.2a2 predominated. VE against 3C.2a1b in 2017-2018 was 37% (95% CI, -57% to 75%), lower at 12% (95% CI, -129% to 67%) for a new 3C.2a1b subcluster (n = 28) also bearing T135K.
Conclusions: Exploring VE by phylogenetic subcluster and prior vaccination history reveals informative heterogeneity. Pivotal mutations affecting glycosylation sites, and repeat vaccination using unchanged antigen, may reduce VE.
Keywords: A(H3N2); genomics; influenza vaccine; influenza virus; subtype; vaccine effectiveness.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures


References
-
- Public Health Agency of Canada (PHAC). Weekly influenza reports. Ottawa: PHAC. https://www.canada.ca/en/public-health/services/diseases/flu-influenza/i.... Accessed 2 October 2019.
-
- Centers for Disease Control and Prevention (CDC). FluView: Weekly U.S. influenza surveillance report. Atlanta, GA: CDC. https://www.cdc.gov/flu/weekly/. Accessed 2 October 2019.
-
- Centers for Disease Control and Prevention (CDC). How CDC classifies flu severity. Atlanta, GA: CDC. https://www.cdc.gov/flu/about/classifies-flu-severity.htm. Accessed 2 October 2019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
