

Association Between Adherence to Evidence-Based Practices for Treatment of Patients With Traumatic Rib Fractures and Mortality Rates Among US Trauma Centers
- PMID: 32215632
- PMCID: PMC7707110
- DOI: 10.1001/jamanetworkopen.2020.1316
Association Between Adherence to Evidence-Based Practices for Treatment of Patients With Traumatic Rib Fractures and Mortality Rates Among US Trauma Centers
Abstract
Importance: Rib fractures are sustained by nearly 15% of patients who experience trauma and are associated with significant morbidity and mortality. Evidence-based practice (EBP) rib fracture management guidelines and treatment algorithms have been published. However, few studies have evaluated trauma center adherence to EBP or the clinical outcomes of each practice within a national cohort.
Objective: To examine adherence to 6 EBPs for rib fractures across US trauma centers and the association with in-hospital mortality.
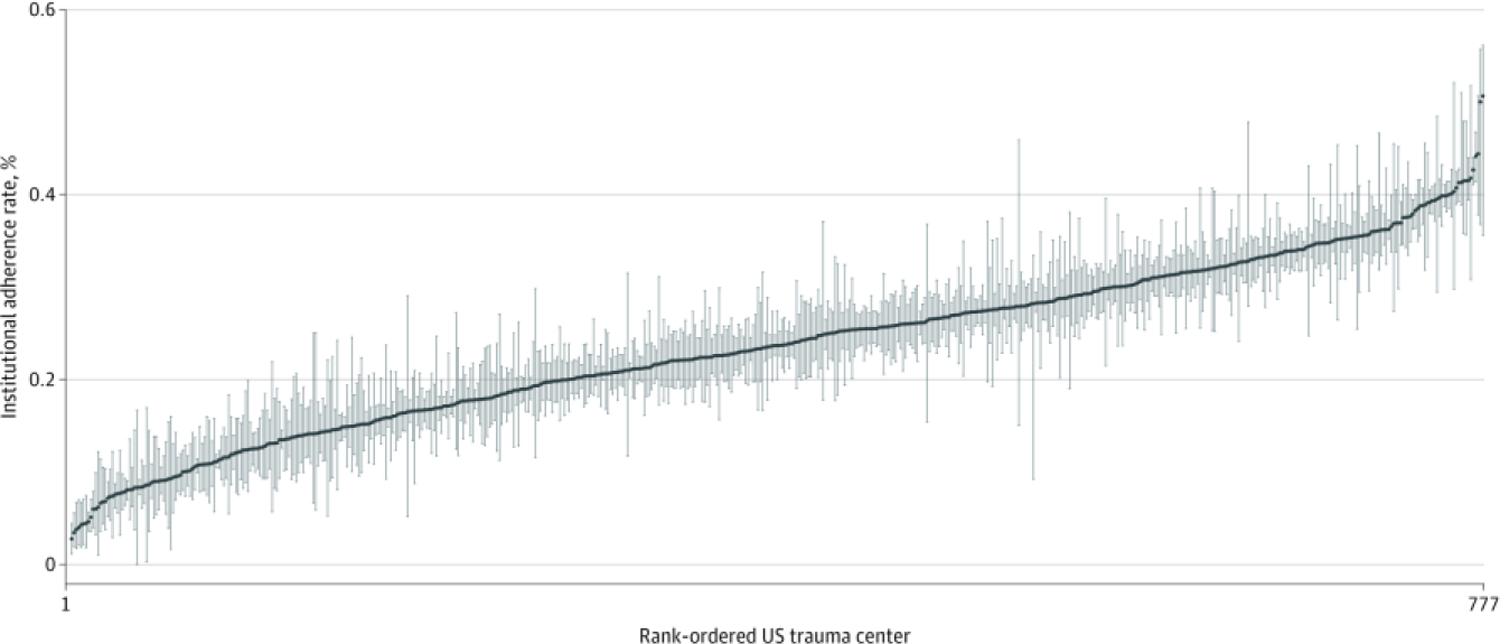
Design, setting, and participants: A retrospective cohort study was conducted from January 1, 2007, to December 31, 2014, of 777 US trauma centers participating in the National Trauma Data Bank. A total of 625 617 patients (age, ≥16 years) were evaluated. Patients without rib fractures and those with no signs of life or institutions with poor data quality were excluded. Data analysis was performed from January 1, 2007, to December 31, 2014.
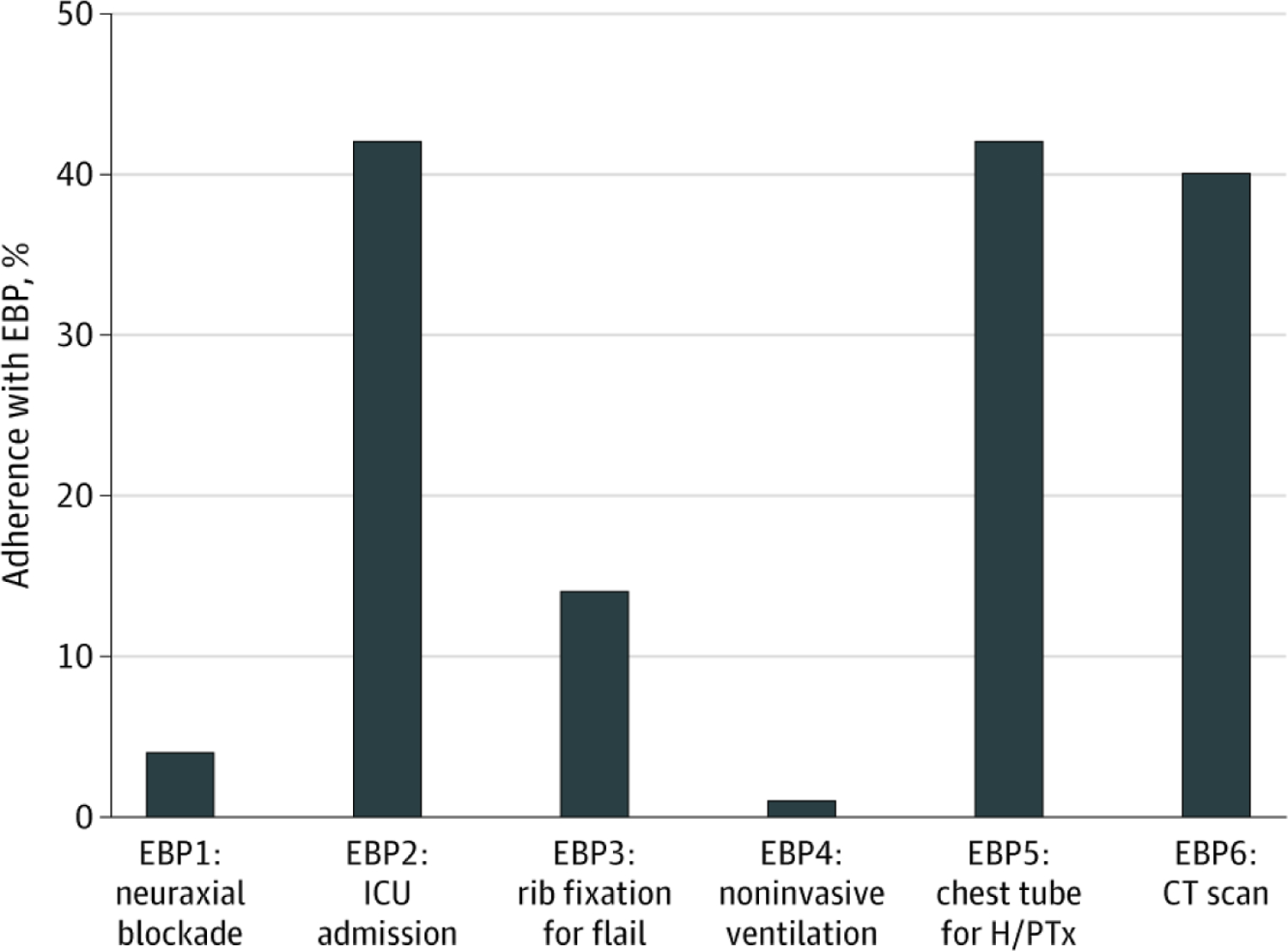
Main outcomes and measures: Six EBPs were defined: (1) neuraxial blockade, (2) intensive care unit admission, (3) pneumatic stabilization, (4) chest computed tomographic scans for older adults (≥65 years) with 3 or more rib fractures, (5) surgical rib fixation for flail chest, and (6) tube thoracostomy placement for hemothorax and/or pneumothorax. Multiple imputation was used to account for missing data. Patients were propensity score matched in a 1:1 fashion based on demographic characteristics; injury severity parameters, including the Injury Severity Score (range, 0-75; higher scores indicate more severe injuries); and comorbidities. Logistic regression was used to determine the association of each practice with all-cause in-hospital mortality.
Results: Of the 625 617 patients with rib fractures included in this analysis, 456 196 patients (73%) were white and 432 229 patients (69%) were male; the median age of the patients was 51 (interquartile range, 37-65) years, and the mean (SD) Injury Severity Score was 18.3 (11.1). The mean (SD) number of rib fractures was 4.2 (2.6). On univariate analysis, patients treated at verified level I trauma centers were more likely to receive 5 or 6 EBPs (all but pneumatic stabilization). Of those who met eligibility, only 4578 of 111 589 patients (4%) received neuraxial blockade, 46 456 of 111 589 patients (42%) were admitted to the intensive care unit, 3302 of 24 319 patients (14%) received surgical rib fixation, 1240 of 111 589 patients (1%) received pneumatic stabilization, 109 160 of 258 334 patients (42%) received tube thoracostomy, and 32 405 of 81 417 patients (40%) received chest computed tomographic scans. Three EBPs were associated with decreased mortality: neuraxial blockade (odds ratio [OR], 0.64; 95% CI, 0.51-0.79; P < .001) for patients aged 65 years or older with 3 or more rib fractures, surgical rib fixation (OR, 0.13; 95% CI, 0.01-0.18; P < .001), and intensive care unit admission (OR, 0.93; 95% CI, 0.86-1.00; P = .04) for patients aged 65 years or older with 3 or more rib fractures. Pneumatic stabilization (OR, 1.71; 95% CI, 1.25-2.35; P < .001) and chest tube placement (OR, 1.27; 95% CI, 1.21-1.33; P < .001) were associated with increased mortality in older patients with 3 or more rib fractures. On multivariable analysis, insurance status, race/ethnicity, injury severity, hospital bed size, and trauma center verification level were associated with receiving EBPs for rib fractures.
Conclusions and relevance: Significant variation appears to exist in the delivery of EBPs for rib fractures across US trauma centers. Three EBPs were associated with reduced mortality, but EBP adherence was poor. Multiple factors, including trauma center verification level, appear to be associated with patients receiving EBPs for rib fractures.
Conflict of interest statement
Figures
Comment in
-
Rib Fractures, the Evidence Supporting Their Management, and Adherence to That Evidence Base.JAMA Netw Open. 2020 Mar 2;3(3):e201591. doi: 10.1001/jamanetworkopen.2020.1591. JAMA Netw Open. 2020. PMID: 32215630 No abstract available.
References
-
- Sharma OP, Oswanski MF, Jolly S, Lauer SK, Dressel R, Stombaugh HA. Perils of rib fractures. Am Surg 2008;74 (4):310–314. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
