

Cost-effectiveness of Mifepristone Pretreatment for the Medical Management of Nonviable Early Pregnancy: Secondary Analysis of a Randomized Clinical Trial
- PMID: 32215633
- PMCID: PMC7439768
- DOI: 10.1001/jamanetworkopen.2020.1594
Cost-effectiveness of Mifepristone Pretreatment for the Medical Management of Nonviable Early Pregnancy: Secondary Analysis of a Randomized Clinical Trial
Abstract
Importance: Early pregnancy loss (EPL) is the most common complication of pregnancy. A multicenter randomized clinical trial compared 2 strategies for medical management and found that mifepristone pretreatment is 25% more effective than the standard of care, misoprostol alone. The cost of mifepristone may be a barrier to implementation of the regimen.
Objective: To assess the cost-effectiveness of medical management of EPL with mifepristone pretreatment plus misoprostol vs misoprostol alone in the United States.
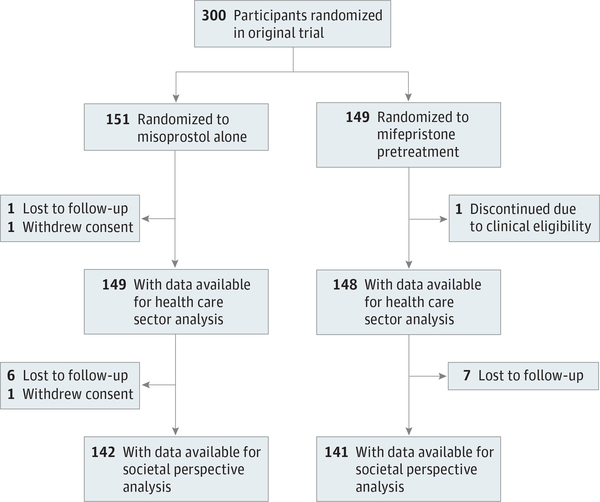
Design, setting, and participants: This preplanned. prospective economic evaluation was performed concurrently with a randomized clinical trial in 3 US sites from May 1, 2014, through April 30, 2017. Participants included 300 women with anembryonic gestation or embryonic or fetal demise. Cost-effectiveness was computed from the health care sector and societal perspectives, with a 30-day time horizon. Data were analyzed from July 1, 2018, to July 3, 2019.
Interventions: Mifepristone pretreatment plus misoprostol administration vs misoprostol alone.
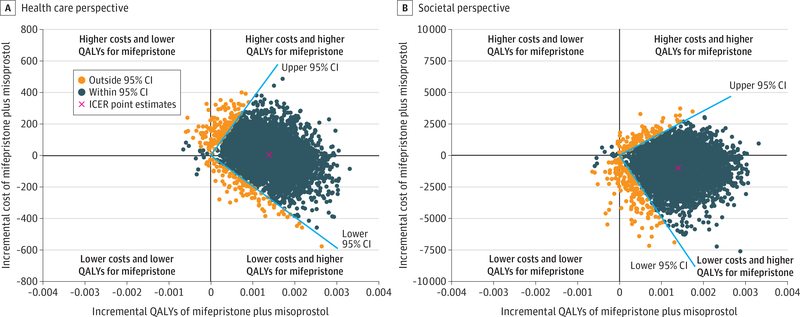
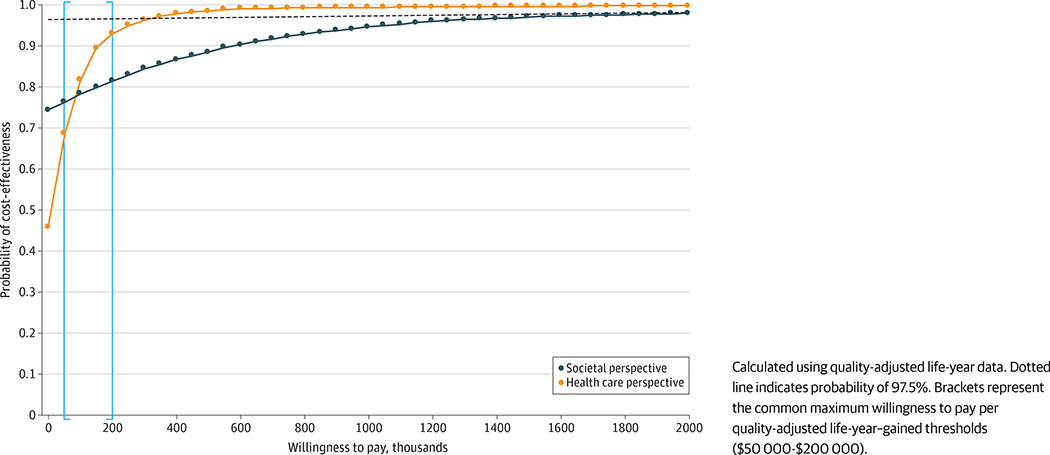
Main outcomes and measures: Costs in 2018 US dollars, effectiveness in quality-adjusted life-years (QALYs), and treatment efficacy. Incremental cost-effectiveness ratios (ICERs) of mifepristone and misoprostol vs misoprostol alone were calculated, and cost-effectiveness acceptability curves were generated.
Results: Among the 300 women included in the randomized clinical trial (mean [SD] age, 30.4 [6.2] years), mean costs were similar for groups receiving mifepristone pretreatment and misoprostol alone from the health care sector perspective ($696.75 [95% CI, $591.88-$801.62] vs $690.88 [95% CI, $562.38-$819.38]; P = .94) and the societal perspective ($3846.30 [95% CI, $2783.01-$4909.58] vs $4845.62 [95% CI, $3186.84-$6504.41]; P = .32). The mifepristone pretreatment group had higher QALYs (0.0820 [95% CI, 0.0815-0.0825] vs 0.0806 [95% CI, 0.0800-0.0812]; P = .001) and a higher completion rate after first treatment (83.8% vs 67.1%; P < .001) than the group receiving misoprostol alone. From the health care sector perspective, mifepristone pretreatment was cost-effective relative to misoprostol alone with an ICER of $4225.43 (95% CI, -$195 053.30 to $367 625.10) per QALY gained. From the societal perspective, mifepristone pretreatment dominated misoprostol alone (95% CI, -$5 111 629 to $1 801 384). The probabilities that mifepristone pretreatment was cost-effective compared with misoprostol alone at a willingness-to-pay of $150 000 per QALY gained from the health care sector and societal perspectives were approximately 90% and 80%, respectively.
Conclusions and relevance: This study found that medical management of EPL with mifepristone pretreatment was cost-effective when compared with misoprostol alone.
Trial registration: ClinicalTrials.gov Identifier: NCT02012491.
Conflict of interest statement
Figures
References
-
- Ventura SJ, Curtin SC, Abma JC, Henshaw SK. Estimated pregnancy rates and rates of pregnancy outcomes for the United States, 1990–2008. Natl Vital Stat Rep. 2012;60(7):1–21. - PubMed
-
- Zhang J, Gilles JM, Barnhart K, Creinin MD, Westhoff C, Frederick MM; National Institute of Child Health Human Development (NICHD) Management of Early Pregnancy Failure Trial. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353(8):761–769. doi: 10.1056/NEJMoa044064 - DOI - PubMed
