

CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19)
- PMID: 32215691
- PMCID: PMC7095246
- DOI: 10.1007/s00330-020-06817-6
CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19)
Abstract
Objectives: To explore the relationship between the imaging manifestations and clinical classification of COVID-19.
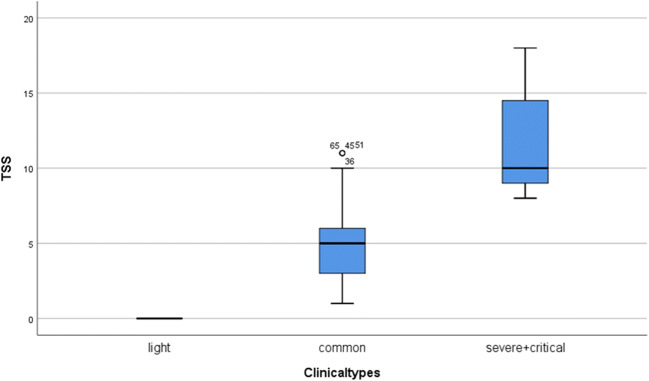
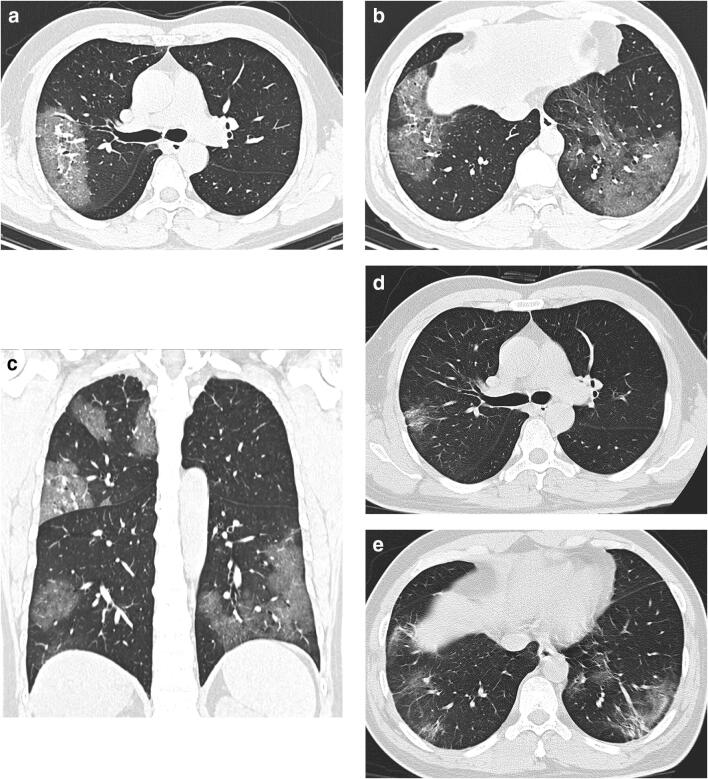
Methods: We conducted a retrospective single-center study on patients with COVID-19 from Jan. 18, 2020 to Feb. 7, 2020 in Zhuhai, China. Patients were divided into 3 types based on Chinese guideline: mild (patients with minimal symptoms and negative CT findings), common, and severe-critical (patients with positive CT findings and different extent of clinical manifestations). CT visual quantitative evaluation was based on summing up the acute lung inflammatory lesions involving each lobe, which was scored as 0 (0%), 1 (1-25%), 2 (26-50%), 3 (51-75%), or 4 (76-100%), respectively. The total severity score (TSS) was reached by summing the five lobe scores. The consistency of two observers was evaluated. The TSS was compared with the clinical classification. ROC was used to test the diagnosis ability of TSS for severe-critical type.
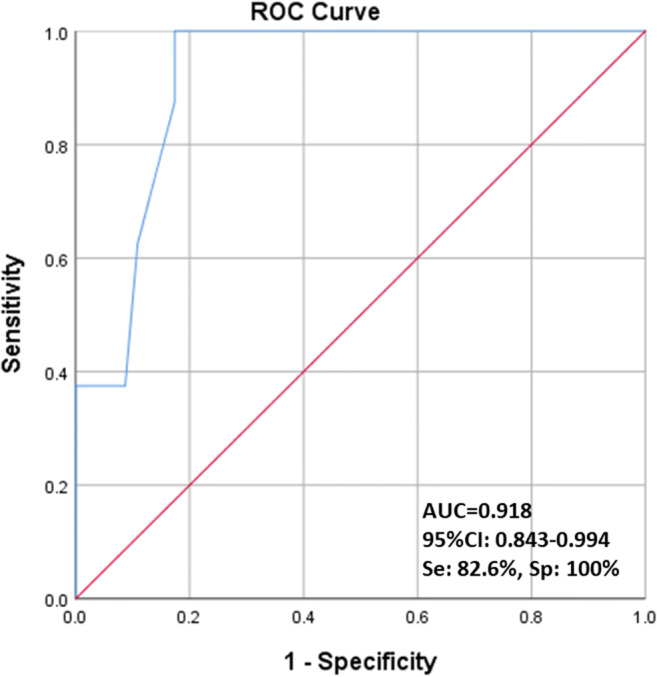
Results: This study included 78 patients, 38 males and 40 females. There were 24 mild (30.8%), 46 common (59.0%), and 8 severe-critical (10.2%) cases, respectively. The median TSS of severe-critical-type group was significantly higher than common type (p < 0.001). The ICC value of the two observers was 0.976 (95% CI 0.962-0.985). ROC analysis showed the area under the curve (AUC) of TSS for diagnosing severe-critical type was 0.918. The TSS cutoff of 7.5 had 82.6% sensitivity and 100% specificity.
Conclusions: The proportion of clinical mild-type patients with COVID-19 was relatively high; CT was not suitable for independent screening tool. The CT visual quantitative analysis has high consistency and can reflect the clinical classification of COVID-19.
Key points: • CT visual quantitative evaluation has high consistency (ICC value of 0.976) among the observers. The median TSS of severe-critical type group was significantly higher than common type (p < 0.001). • ROC analysis showed the area under the curve (AUC) of TSS for diagnosing severe-critical type was 0.918 (95% CI 0.843-0.994). The TSS cutoff of 7.5 had 82.6% sensitivity and 100% specificity. • The proportion of confirmed COVID-19 patients with normal chest CT was relatively high (30.8%); CT was not a suitable screening modality.
Keywords: COVID-19; Classification; Quantitative evaluation; Tomography, X-ray computed.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
-
- Zhu N, Zhang D, Wang W et al (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 10.1056/NEJMoa2001017 - PubMed
-
- WHO main website. https://www.who.int. Accessed March 12th, 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
