

Design, Implementation, and Validation of a Pediatric ICU Sepsis Prediction Tool as Clinical Decision Support
- PMID: 32215893
- PMCID: PMC7096320
- DOI: 10.1055/s-0040-1705107
Design, Implementation, and Validation of a Pediatric ICU Sepsis Prediction Tool as Clinical Decision Support
Abstract
Background: Sepsis is an uncontrolled inflammatory reaction caused by infection. Clinicians in the pediatric intensive care unit (PICU) developed a paper-based tool to identify patients at risk of sepsis. To improve the utilization of the tool, the PICU team integrated the paper-based tool as a real-time clinical decision support (CDS) intervention in the electronic health record (EHR).
Objective: This study aimed to improve identification of PICU patients with sepsis through an automated EHR-based CDS intervention.
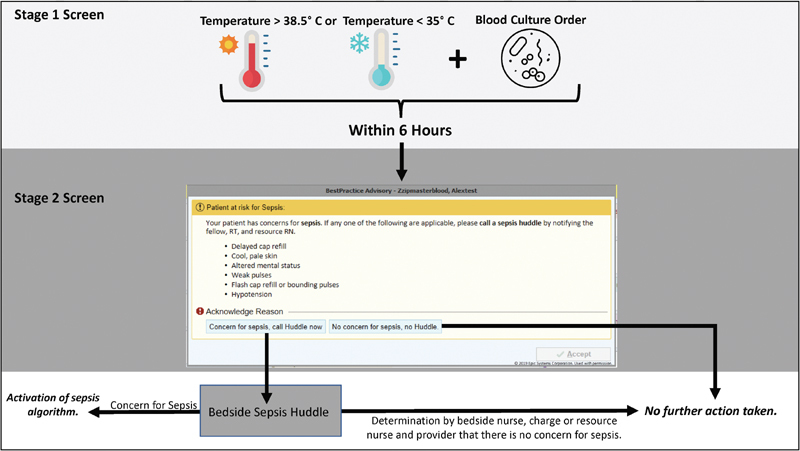
Methods: A prospective cohort study of all patients admitted to the PICU from May 2017 to May 2019. A CDS intervention was implemented in May 2018. The CDS intervention screened patients for nonspecific sepsis criteria, temperature dysregulation and a blood culture within 6 hours. Following the screening, an interruptive alert prompted nursing staff to complete a perfusion screen to assess for clinical signs of sepsis. The primary alert performance outcomes included sensitivity, specificity, and positive and negative predictive value. The secondary clinical outcome was completion of sepsis management tasks.
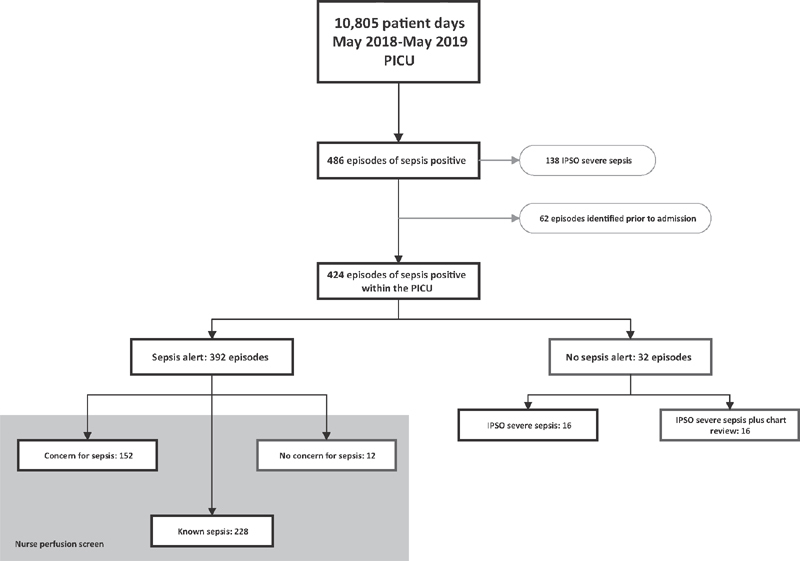
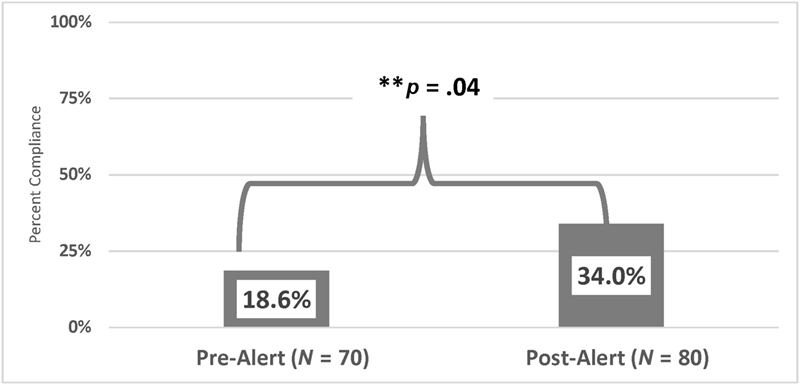
Results: During the 1-year post implementation period, there were 45.0 sepsis events per 1,000 patient days over 10,805 patient days. The sepsis alert identified 392 of the 436 sepsis episodes accurately with sensitivity of 92.5%, specificity of 95.6%, positive predictive value of 46.0%, and negative predictive value of 99.7%. Examining only patients with severe sepsis confirmed by chart review, test characteristics fell to a sensitivity of 73.3%, a specificity of 92.5%. Prior to the initiation of the alert, 18.6% (13/70) of severe sepsis patients received recommended sepsis interventions. Following the implementation, 34% (27/80) received these interventions in the time recommended, p = 0.04.
Conclusion: An EHR CDS intervention demonstrated strong performance characteristics and improved completion of recommended sepsis interventions.
Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
None declared.
Figures
References
-
- Despond O, Proulx F, Carcillo J A, Lacroix J. Pediatric sepsis and multiple organ dysfunction syndrome. Curr Opin Pediatr. 2001;13(03):247–253. - PubMed
-
- DuPont H L, Spink W W. Infections due to gram-negative organisms: an analysis of 860 patients with bacteremia at the University of Minnesota Medical Center, 1958-1966. Medicine (Baltimore) 1969;48(04):307–332. - PubMed
-
- Hartman M E, Linde-Zwirble W T, Angus D C, Watson R S. Trends in the epidemiology of pediatric severe sepsis*. Pediatr Crit Care Med. 2013;14(07):686–693. - PubMed
-
- Han Y Y, Carcillo J A, Dragotta M A et al.Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics. 2003;112(04):793–799. - PubMed
