

Anti-vimentin antibodies: a unique antibody class associated with therapy-resistant lupus nephritis
- PMID: 32216516
- PMCID: PMC7278023
- DOI: 10.1177/0961203320913606
Anti-vimentin antibodies: a unique antibody class associated with therapy-resistant lupus nephritis
Abstract
Background:: Tubulointerstitial inflammation (TII) in lupus nephritis (LN) is associated with a worse prognosis. Vimentin, a filamental antigen, is commonly targeted by in situ activated B-cells in TII. The prognostic importance of high serum anti-vimentin antibodies (AVAs) in LN and their relationship with common lupus autoantibody specificities is unknown. Herein we investigated associations between AVA isotypes, other autoantibodies, and response to mycophenolate mofetil (MMF) in the presence or absence of rituximab.
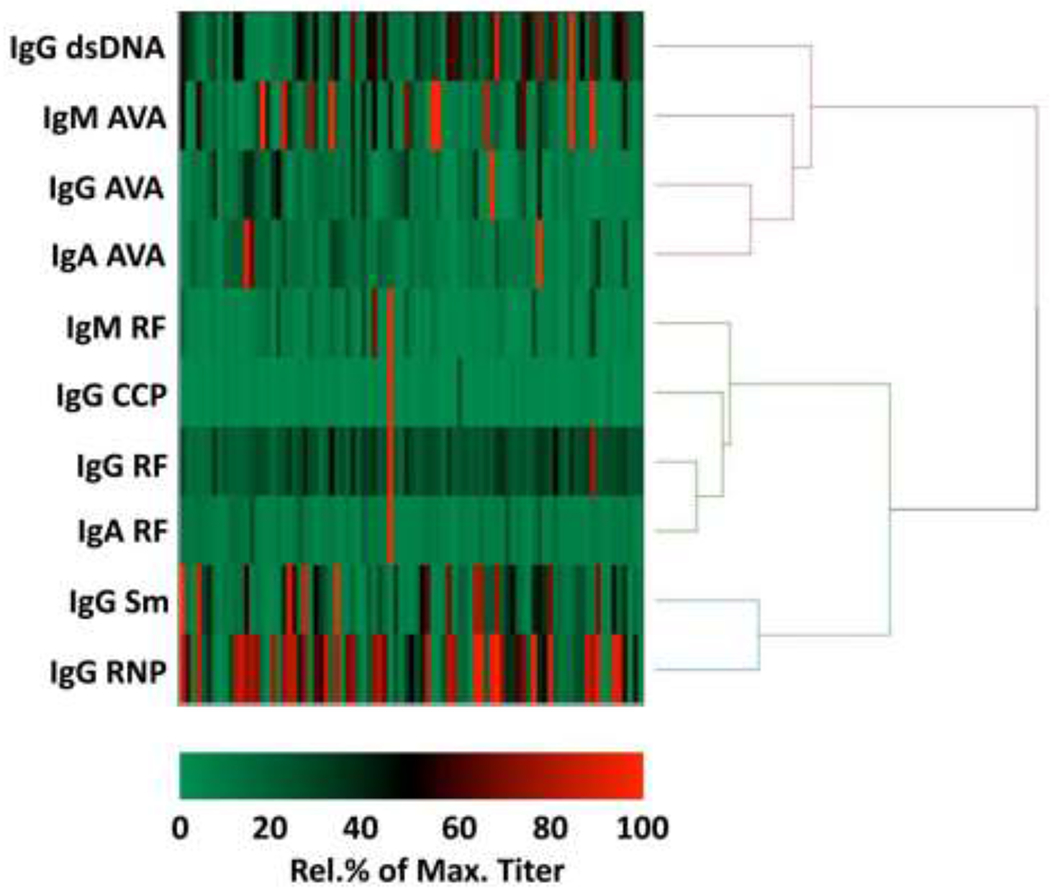
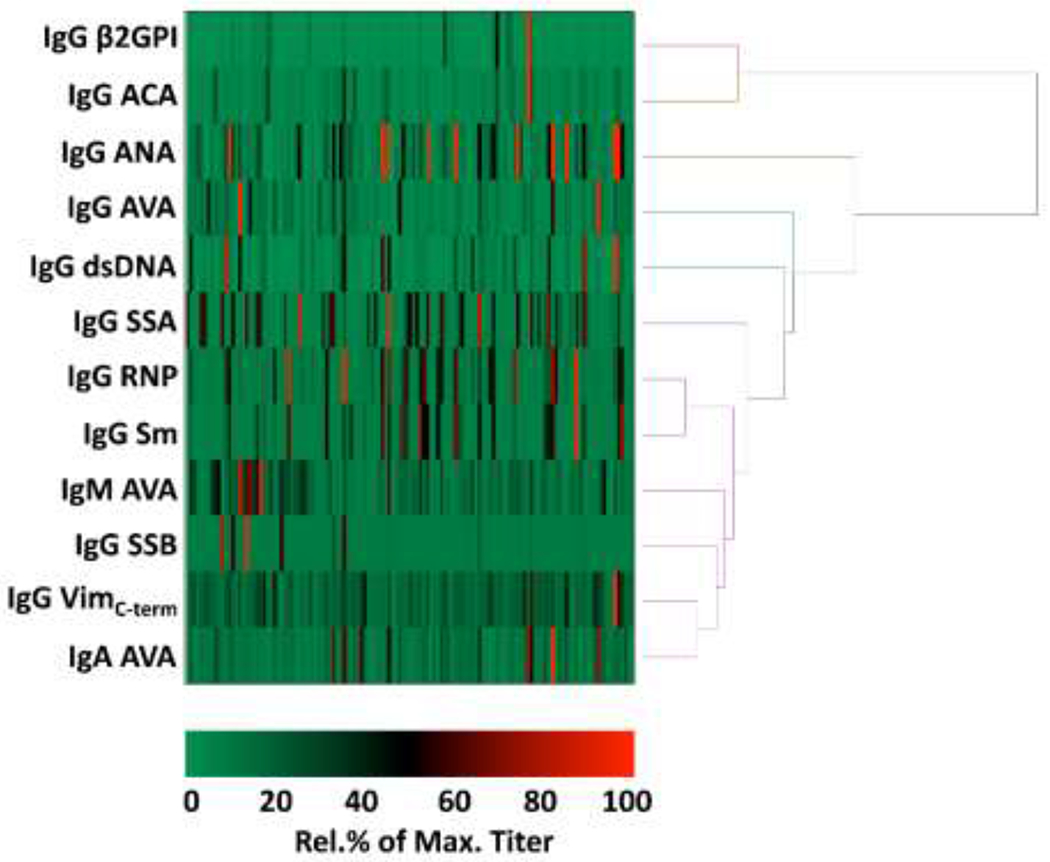
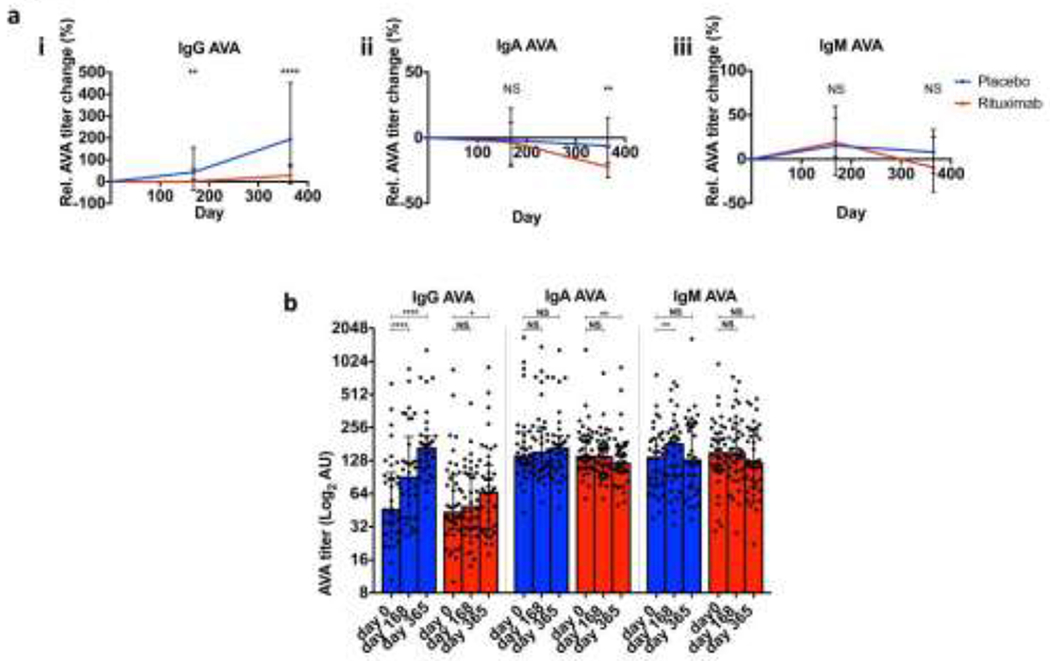
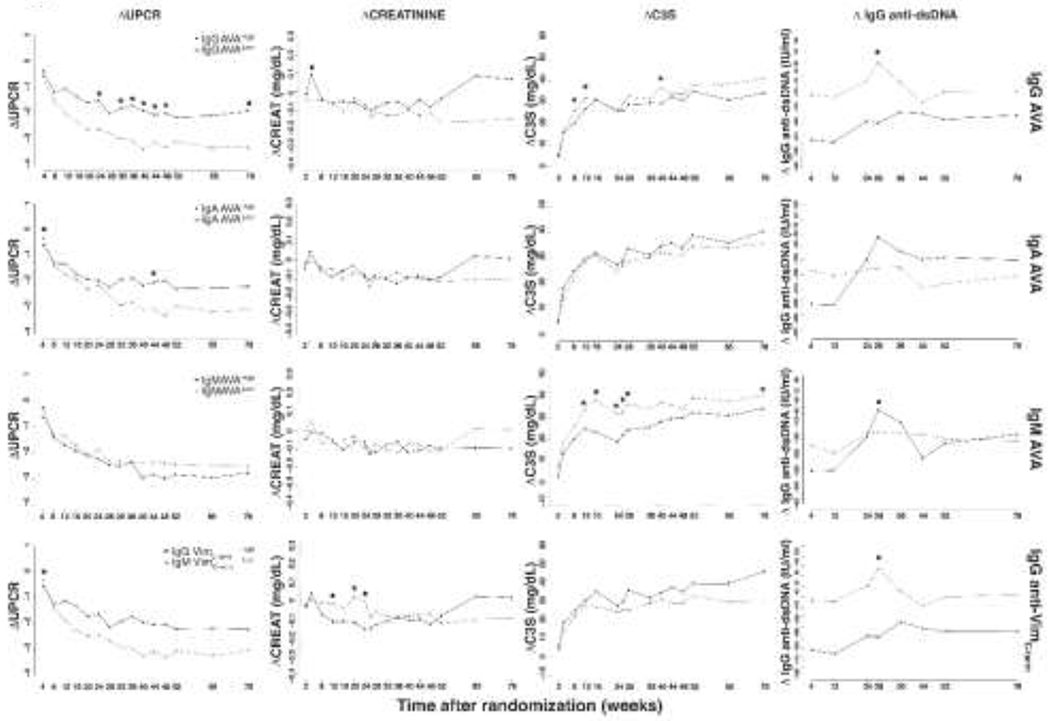
Methods:: The Translational Research Inititative in the Department of Medicine (TRIDOM) cross-sectional cohort of 99 lupus patients was assayed for IgG-, IgA- and IgM- AVAs, lupus associated and rheumatoid arthritis (RA) associated antibodies, and hierarchically clustered. Serum from baseline, 26 and 52 weeks from 132 LUNAR trial enrolled LN patients was also analysed and correlated with renal function up to week 78.
Results:: In TRIDOM, AVAs, especially IgM AVAs, clustered with IgG anti-dsDNA and away from anti-Sm and -RNP and RA associated antibodies. In LUNAR at baseline, AVAs correlated weakly with anti-dsDNA and more strongly with anti-cardiolipin titres. Regardless of treatment, IgG-, but not IgM- or IgA-, AVAs were higher at week 52 than at baseline. In contrast, anti-dsDNA titres declined, regardless of therapeutic regime. High IgG AVA titres at entry predicted less response to therapy.
Conclusion:: AVAs, especially IgG AVAs, are unique in distribution and response to therapy compared to other commonly measured autoantibody specificities. Furthermore, high-titre IgG AVAs identify LN patients resistant to conventional therapies. These data suggest that AVAs represent an independent class of prognostic autoantibodies.
Keywords: Vimentin; autoantibodies; lupus nephritis; prognosis; systemic lupus erythematosus.
Conflict of interest statement
COMPETING INTERESTS:
MC, JD & MJT are employee of Roche/Genentech. LLD is an employee of Janssen Biopharma which is part of the Johnson and Johnson family of companies. All other authors have nothing to disclose
Figures
Similar articles
-
Editorial: autoimmunity to vimentin and lupus nephritis.Arthritis Rheumatol. 2014 Dec;66(12):3251-4. doi: 10.1002/art.38885. Arthritis Rheumatol. 2014. PMID: 25250522 Free PMC article. No abstract available.
-
A Case of NCAM1-Positive Lupus Nephritis with NCAM1 Antibody Titers Responsive to Rituximab.Nephron. 2024;148(5):312-318. doi: 10.1159/000534037. Epub 2023 Sep 29. Nephron. 2024. PMID: 37778328
-
Longterm clinical and immunological effects of anti-CD20 treatment in patients with refractory systemic lupus erythematosus.J Rheumatol. 2008 May;35(5):826-33. Epub 2008 Apr 1. J Rheumatol. 2008. PMID: 18398943
-
Exploring new territory: the move towards individualised treatment.Lupus. 2007;16(3):227-31. doi: 10.1191/0961203306075616. Lupus. 2007. PMID: 17432112 Review.
-
Diagnostic and prognostic significance of anti-C1q antibodies in systemic lupus erythematosus.Curr Opin Nephrol Hypertens. 2003 Nov;12(6):619-24. doi: 10.1097/00041552-200311000-00008. Curr Opin Nephrol Hypertens. 2003. PMID: 14564199 Review.
Cited by
-
Specific in situ inflammatory states associate with progression to renal failure in lupus nephritis.J Clin Invest. 2022 Jul 1;132(13):e155350. doi: 10.1172/JCI155350. J Clin Invest. 2022. PMID: 35608910 Free PMC article.
-
Machine Learning to Quantify In Situ Humoral Selection in Human Lupus Tubulointerstitial Inflammation.Front Immunol. 2020 Nov 27;11:593177. doi: 10.3389/fimmu.2020.593177. eCollection 2020. Front Immunol. 2020. PMID: 33329582 Free PMC article.
-
Cellular aspects of the pathogenesis of lupus nephritis.Curr Opin Rheumatol. 2021 Mar 1;33(2):197-204. doi: 10.1097/BOR.0000000000000777. Curr Opin Rheumatol. 2021. PMID: 33394604 Free PMC article. Review.
-
Generation of Monoclonal Antibodies Specific for Native LL37 and Citrullinated LL37 That Discriminate the Two LL37 Forms in the Skin and Circulation of Cutaneous/Systemic Lupus Erythematosus and Rheumatoid Arthritis Patients.Antibodies (Basel). 2020 May 11;9(2):14. doi: 10.3390/antib9020014. Antibodies (Basel). 2020. PMID: 32403306 Free PMC article.
-
Vimentin as a Multifaceted Player and Potential Therapeutic Target in Viral Infections.Int J Mol Sci. 2020 Jun 30;21(13):4675. doi: 10.3390/ijms21134675. Int J Mol Sci. 2020. PMID: 32630064 Free PMC article. Review.
References
-
- Edelbauer M, Jungraithmayr T, and Zimmerhackl LB, Rituximab in childhood systemic lupus erythematosus refractory to conventional immunosuppression: case report. Pediatr Nephrol, 2005. 20(6): p. 811–3. - PubMed
-
- Fra GP, Avanzi GC, and Bartoli E, Remission of refractory lupus nephritis with a protocol including rituximab. Lupus, 2003. 12(10): p. 783–7. - PubMed
-
- van Vollenhoven RF, et al., Biopsy-verified response of severe lupus nephritis to treatment with rituximab (anti-CD20 monoclonal antibody) plus cyclophosphamide after biopsy-documented failure to respond to cyclophosphamide alone. Scand J Rheumatol, 2004. 33(6): p. 423–7. - PubMed
-
- Condon MB, et al., Prospective observational single-centre cohort study to evaluate the effectiveness of treating lupus nephritis with rituximab and mycophenolate mofetil but no oral steroids. Ann Rheum Dis, 2013. 72(8): p. 1280–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
