

Vascular toxic effects of cancer therapies
- PMID: 32218531
- PMCID: PMC8782612
- DOI: 10.1038/s41569-020-0347-2
Vascular toxic effects of cancer therapies
Abstract
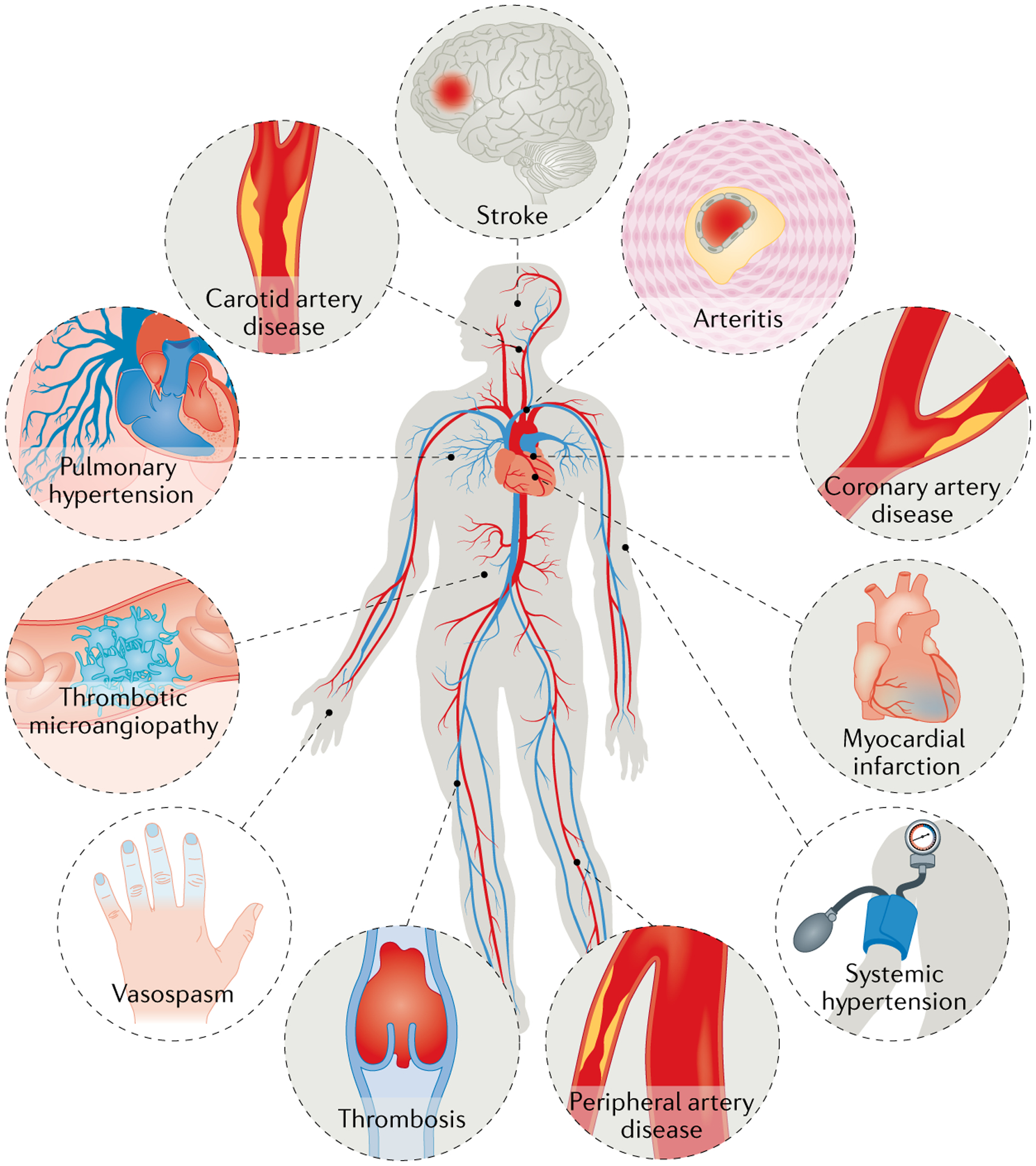
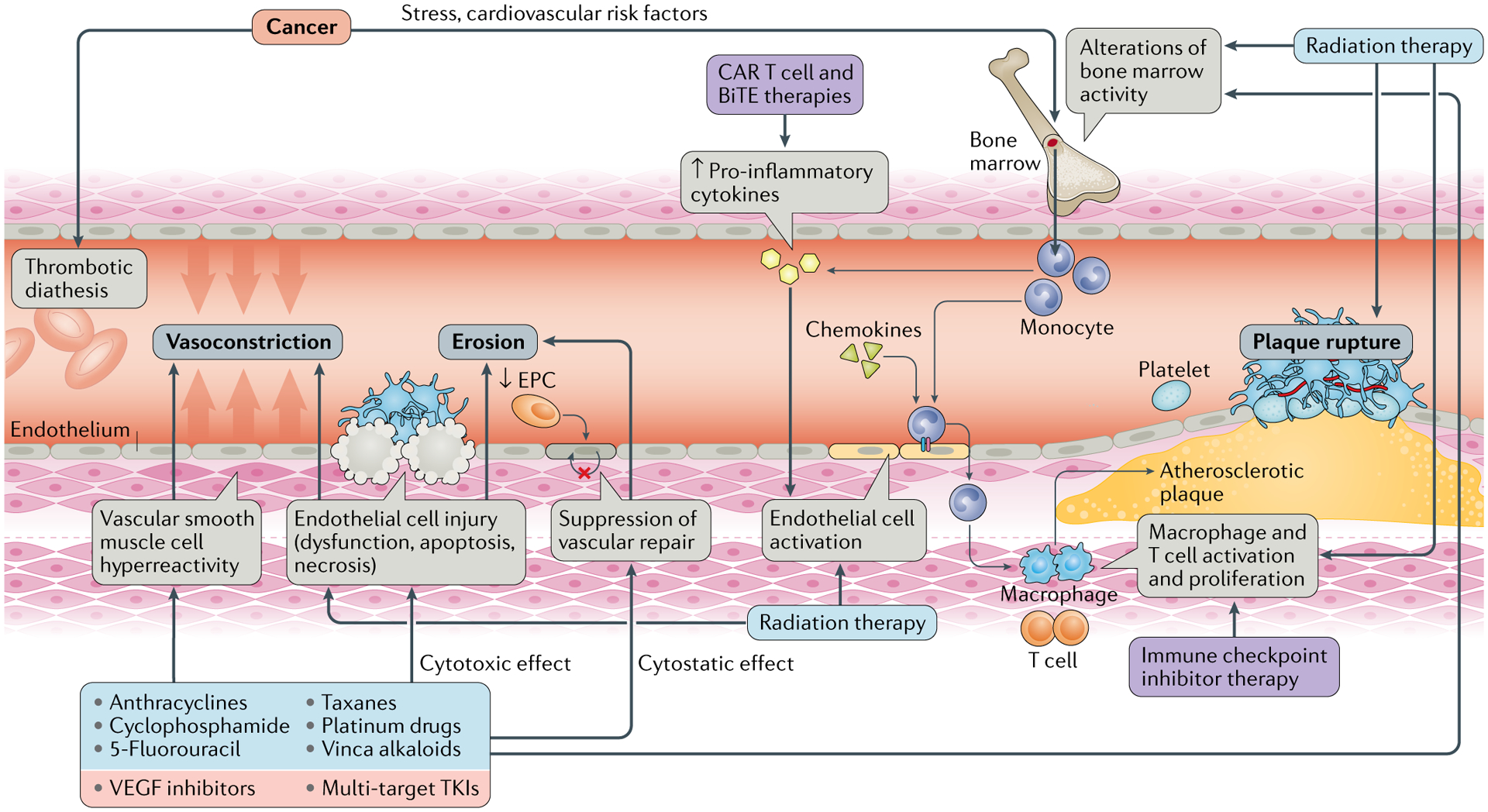
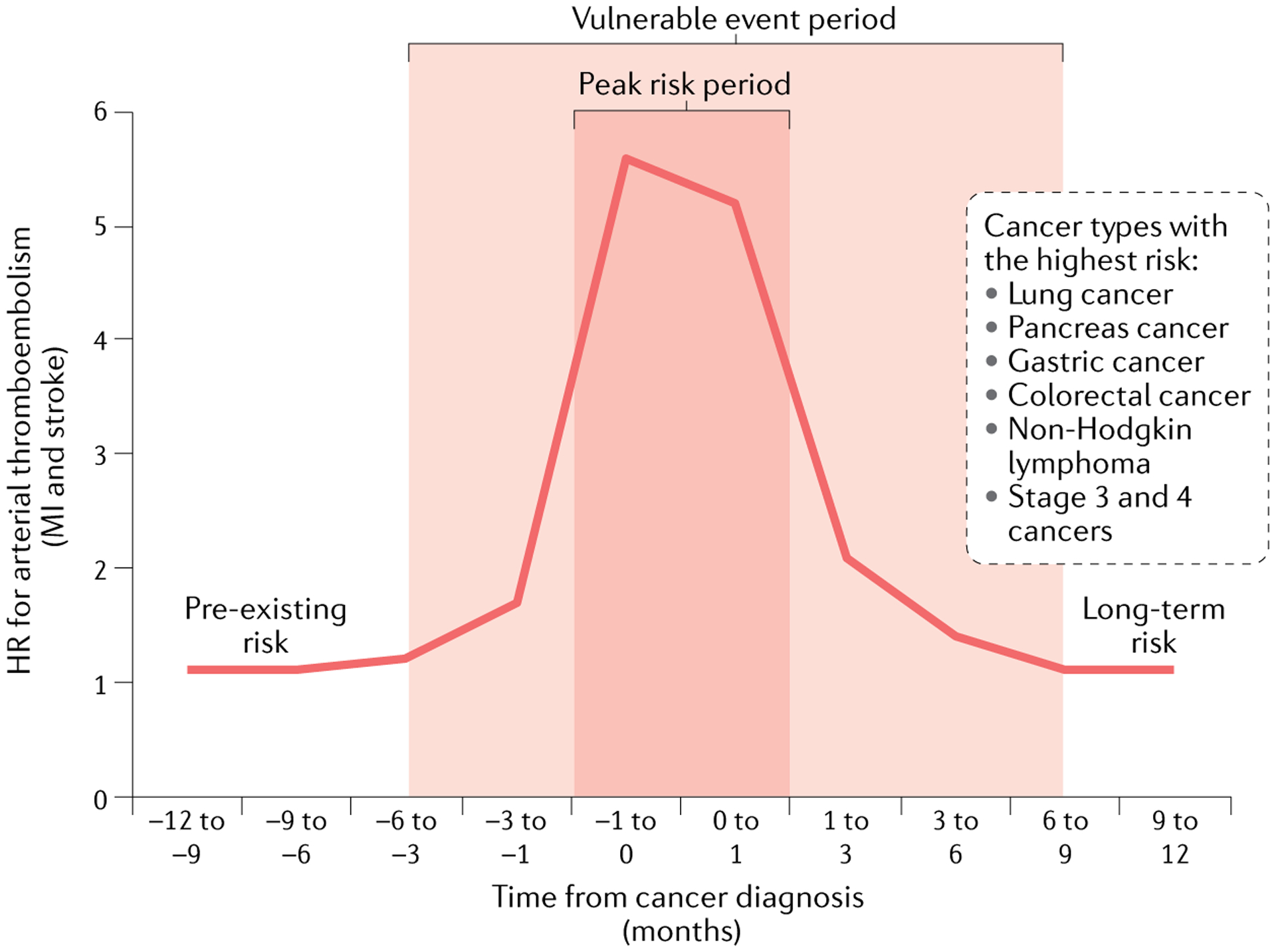
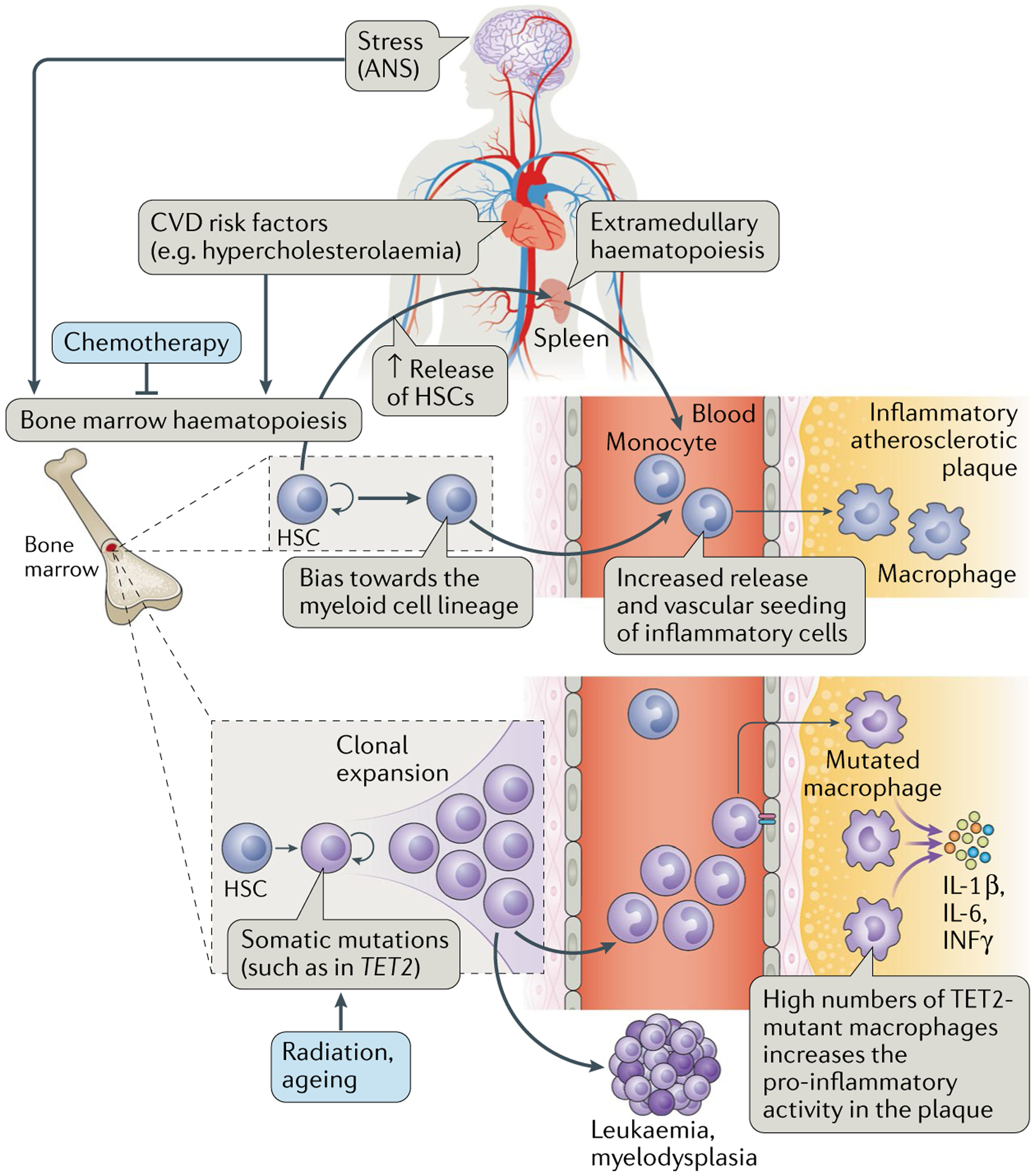
Cancer therapies can lead to a broad spectrum of cardiovascular complications. Among these, cardiotoxicities remain of prime concern, but vascular toxicities have emerged as the second most common group. The range of cancer therapies with a vascular toxicity profile and the clinical spectrum of vascular toxic effects are quite broad. Historically, venous thromboembolism has received the greatest attention but, over the past decade, the arterial toxic effects, which can present as acute vasospasm, acute thrombosis and accelerated atherosclerosis, of cancer therapies have gained greater recognition. This Review focuses on these types of cancer therapy-related arterial toxicity, including their mechanisms, and provides an update on venous thromboembolism and pulmonary hypertension associated with cancer therapies. Recommendations for the screening, treatment and prevention of vascular toxic effects of cancer therapies are outlined in the context of available evidence and society guidelines and consensus statements. The shift towards greater awareness of the vascular toxic effects of cancer therapies has further unveiled the urgent needs in this area in terms of defining best clinical practices. Well-designed and well-conducted clinical studies and registries are needed to more precisely define the incidence rates, risk factors, primary and secondary modes of prevention, and best treatment modalities for vascular toxicities related to cancer therapies. These efforts should be complemented by preclinical studies to outline the pathophysiological concepts that can be translated into the clinic and to identify drugs with vascular toxicity potential even before their widespread clinical use.
Conflict of interest statement
Competing interests
The author declares no competing interests.
Figures
Comment in
-
Apixaban therapy is effective and safe for cancer-associated VTE.Nat Rev Cardiol. 2020 Jun;17(6):322. doi: 10.1038/s41569-020-0386-8. Nat Rev Cardiol. 2020. PMID: 32296144 No abstract available.
-
Rivaroxaban reduces ischaemic events in patients with PAD.Nat Rev Cardiol. 2020 Jun;17(6):322. doi: 10.1038/s41569-020-0385-9. Nat Rev Cardiol. 2020. PMID: 32296145 No abstract available.
References
-
- Kleiman NS, Lehane DE, Geyer CE Jr., Pratt CM & Young JB Prinzmetal’s angina during 5-fluorouracil chemotherapy. Am. J. Med 82, 566–568 (1987). - PubMed
-
- Collins C & Weiden PL Cardiotoxicity of 5-fluorouracil. Cancer Treat. Rep 71, 733–736 (1987). - PubMed
-
- Schnetzler B, Popova N, Collao Lamb C & Sappino AP Coronary spasm induced by capecitabine. Ann. Oncol 12, 723–724 (2001). - PubMed
-
- Mosseri M, Fingert HJ, Varticovski L, Chokshi S & Isner JM In vitro evidence that myocardial ischemia resulting from 5-fluorouracil chemotherapy is due to protein kinase C-mediated vasoconstriction of vascular smooth muscle. Cancer Res. 53, 3028–3033 (1993). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
