

The Impact of Delayed Switch to Second-Line Antiretroviral Therapy on Mortality, Depending on Definition of Failure Time and CD4 Count at Failure
- PMID: 32219384
- PMCID: PMC7523585
- DOI: 10.1093/aje/kwaa049
The Impact of Delayed Switch to Second-Line Antiretroviral Therapy on Mortality, Depending on Definition of Failure Time and CD4 Count at Failure
Abstract
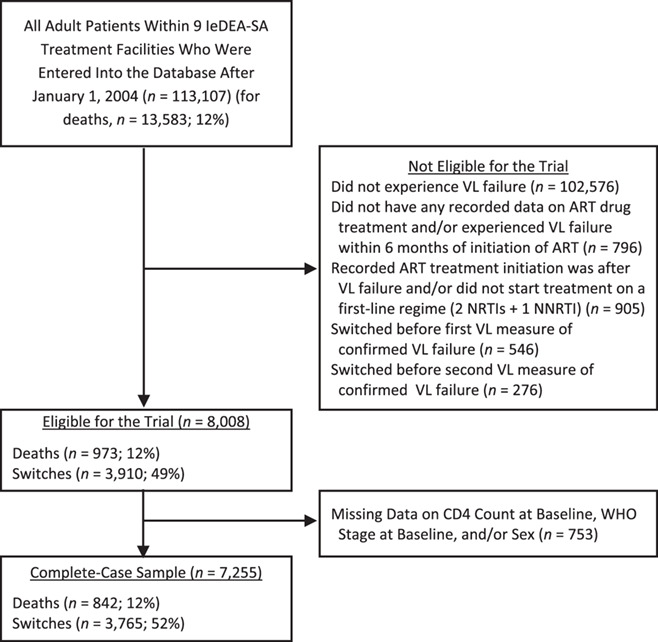
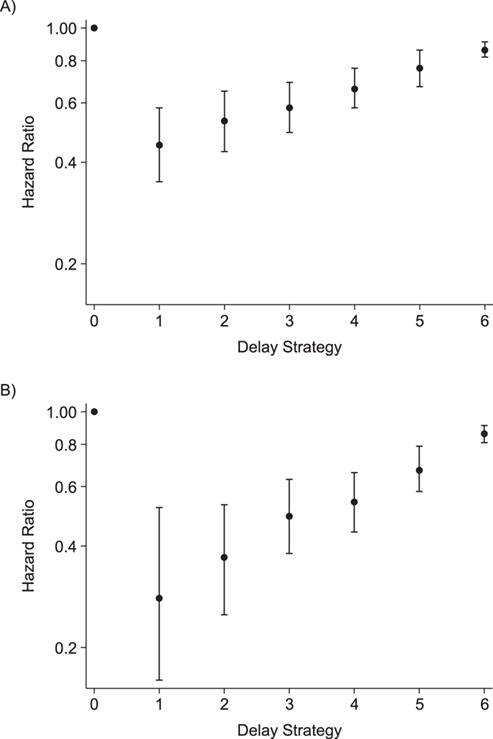
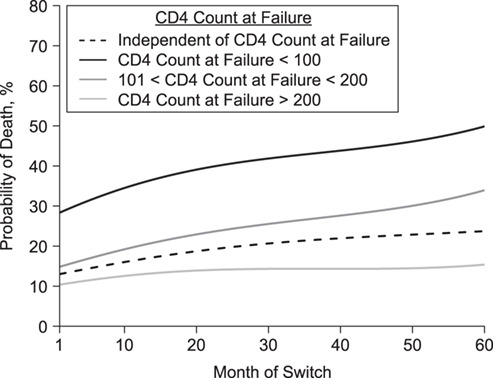
Little is known about the functional relationship of delaying second-line treatment initiation for human immunodeficiency virus-positive patients and mortality, given a patient's immune status. We included 7,255 patients starting antiretroviral therapy during 2004-2017, from 9 South African cohorts, with virological failure and complete baseline data. We estimated the impact of switch time on the hazard of death using inverse probability of treatment weighting of marginal structural models. The nonlinear relationship between month of switch and the 5-year survival probability, stratified by CD4 count at failure, was estimated with targeted maximum likelihood estimation. We adjusted for measured time-varying confounding by CD4 count, viral load, and visit frequency. Five-year mortality was estimated to be 10.5% (95% CI: 2.2, 18.8) for immediate switch and to be 26.6% (95% CI: 20.9, 32.3) for no switch (51.1% if CD4 count was <100 cells/mm3). The hazard of death was estimated to be 0.37 (95% CI: 0.30, 0.46) times lower if everyone had been switched immediately compared with never. The shorter the delay in switching, the lower the hazard of death-delaying 30-59 days reduced the hazard by 0.53 (95% CI: 0.43, 0.65) times and 60-119 days by 0.58 (95% CI: 0.49, 0.69) times, compared with no switch. Early treatment switch is particularly important for patients with low CD4 counts at failure.
Keywords: HIV; causal inference; second-line ART; targeted learning; treatment switching.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- UNAIDS UNAIDS data 2018. https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_.... Accessed March 18, 2020.
-
- Cain LE, Sterne JAC, May MT, et al. . When to switch cART: novel methods for the comparison of switching strategies using observational data. Am J Epidemiol. 2012;175(suppl):S117.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
