

The Effect of Improving Basic Preventive Measures in the Perioperative Arena on Staphylococcus aureus Transmission and Surgical Site Infections: A Randomized Clinical Trial
- PMID: 32219407
- PMCID: PMC11071519
- DOI: 10.1001/jamanetworkopen.2020.1934
The Effect of Improving Basic Preventive Measures in the Perioperative Arena on Staphylococcus aureus Transmission and Surgical Site Infections: A Randomized Clinical Trial
Abstract
Importance: Surgical site infections increase patient morbidity and health care costs. The Centers for Disease Control and Prevention emphasize improved basic preventive measures to reduce bacterial transmission and infections among patients undergoing surgery.
Objective: To assess whether improved basic preventive measures can reduce perioperative Staphylococcus aureus transmission and surgical site infections.
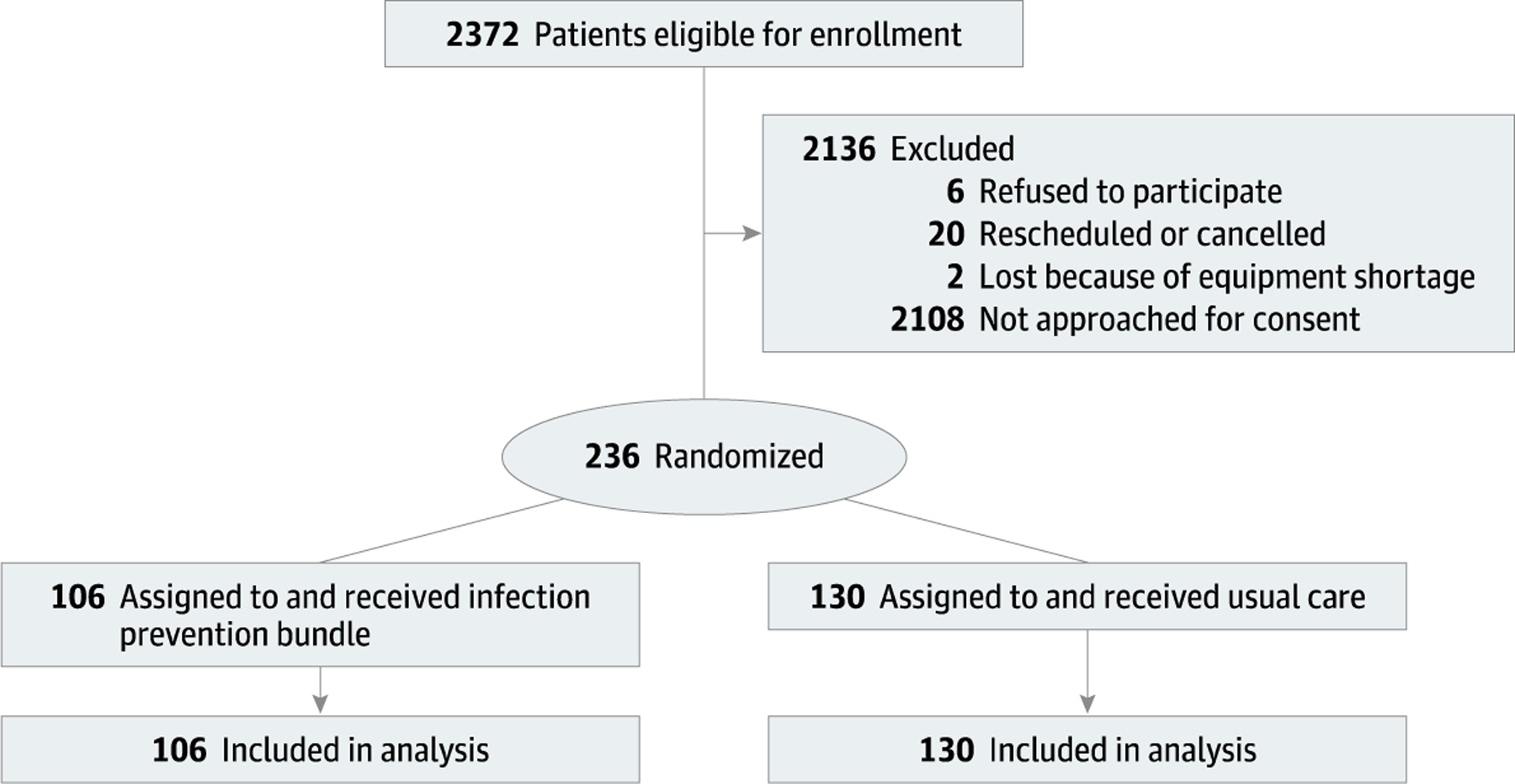
Design, setting, and participants: This randomized clinical trial was conducted from September 20, 2018, to September 20, 2019, among 19 surgeons and their 236 associated patients at a major academic medical center with a 60-day follow-up period. Participants were a random sample of adult patients undergoing orthopedic total joint, orthopedic spine, oncologic gynecological, thoracic, general, colorectal, open vascular, plastic, or open urological surgery requiring general or regional anesthesia. Surgeons and their associated patients were randomized 1:1 via a random number generator to treatment group or to usual care. Observers were masked to patient groupings during assessment of outcome measures.
Interventions: Sustained improvements in perioperative hand hygiene, vascular care, environmental cleaning, and patient decolonization efforts.
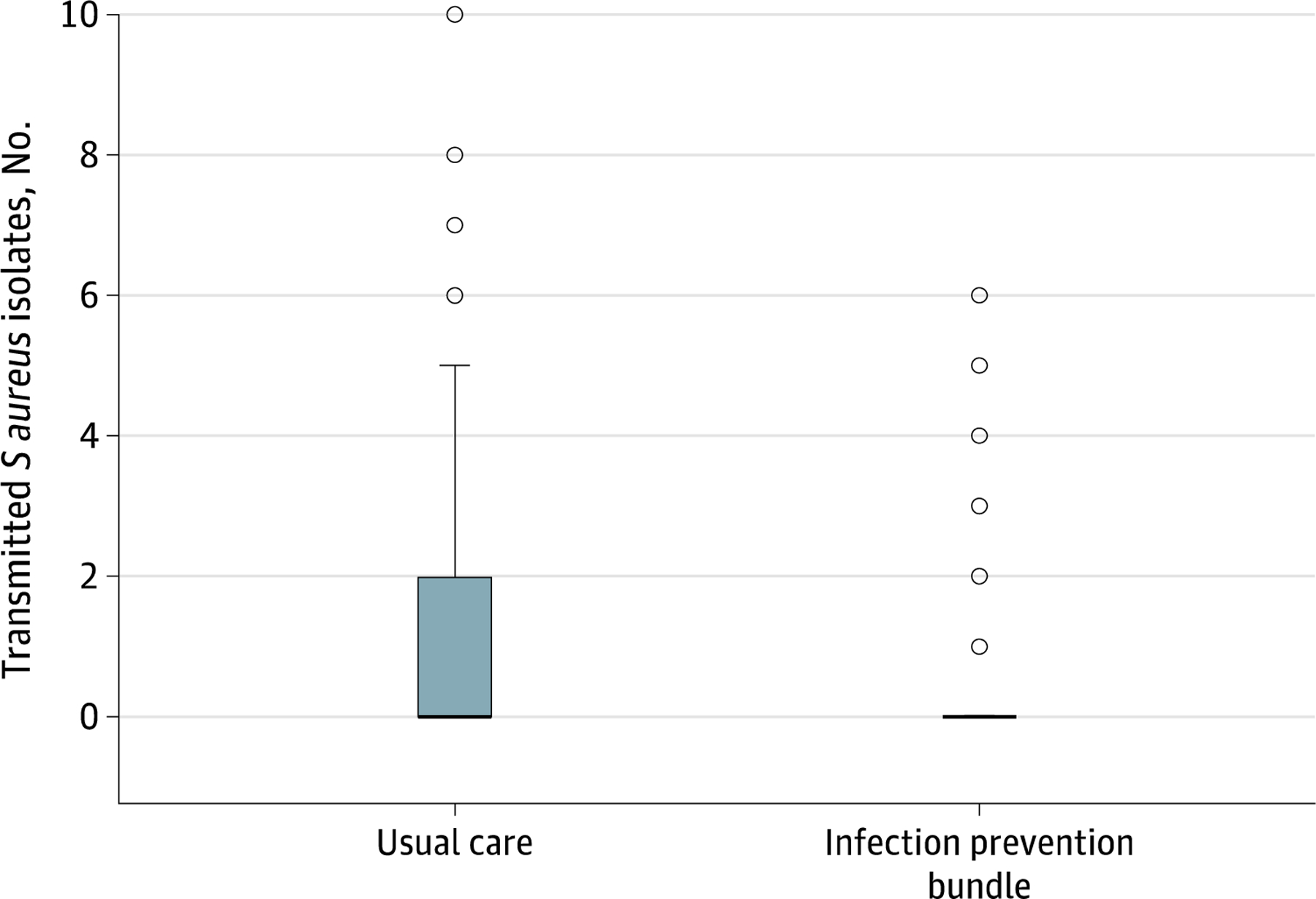
Main outcomes and measures: Perioperative S aureus transmission assessed by the number of isolates transmitted and the incidence of transmission among patient care units (primary) and the incidence of surgical site infections (secondary).
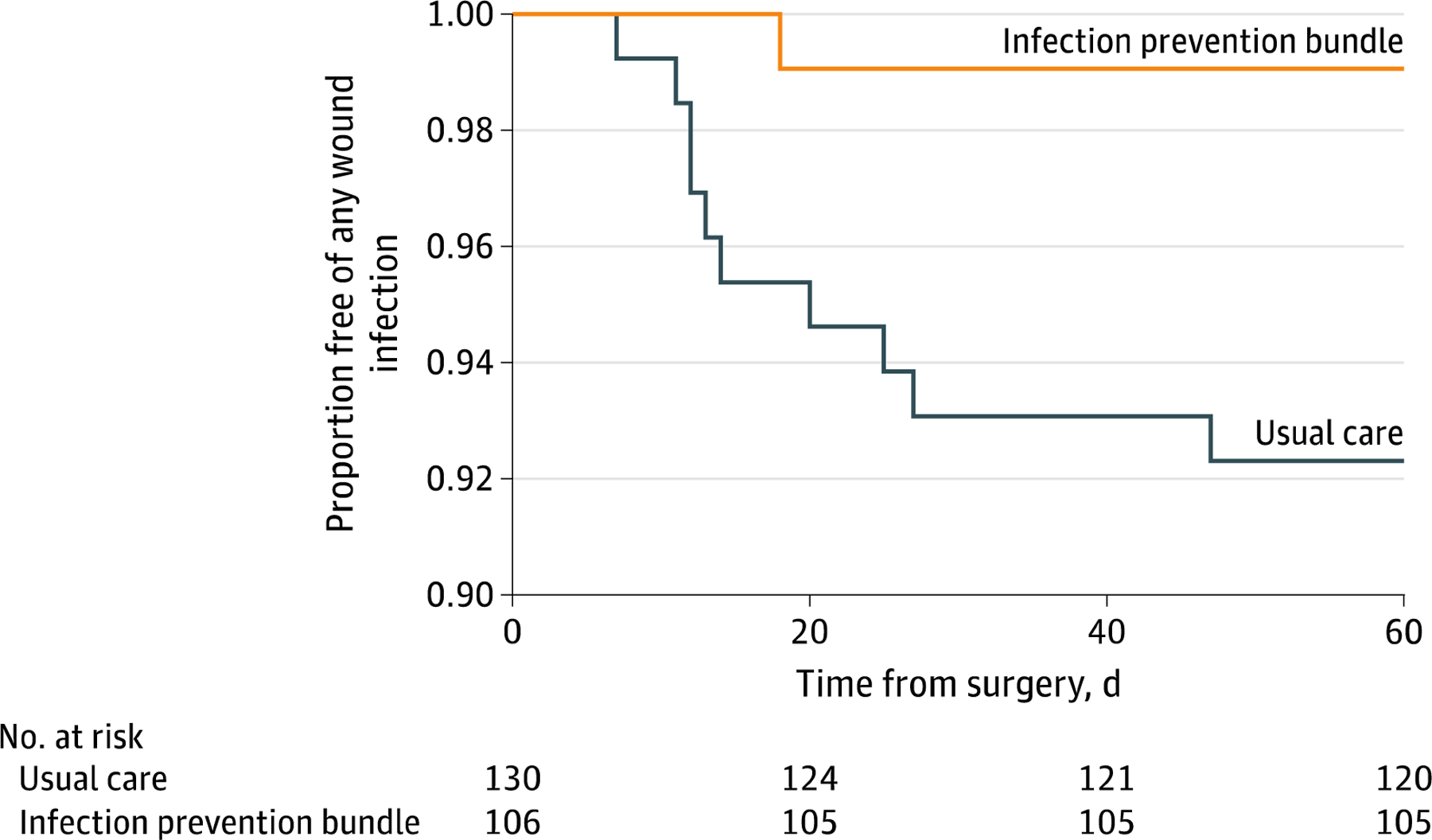
Results: Of 236 patients (156 [66.1%] women; mean [SD] age, 57 [15] years), 106 (44.9%) and 130 (55.1%) were allocated to the treatment and control groups, respectively, received the intended treatment, and were analyzed for the primary outcome. Compared with the control group, the treatment group had a reduced mean (SD) number of transmitted perioperative S aureus isolates (1.25 [2.11] vs 0.47 [1.13]; P = .002). Treatment reduced the incidence of S aureus transmission (incidence risk ratio; 0.56; 95% CI, 0.37-0.86; P = .008; with robust variance clustering by surgeon: 95% CI, 0.42-0.76; P < .001). Overall, 11 patients (4.7%) experienced surgical site infections, 10 (7.7%) in the control group and 1 (0.9%) in the treatment group. Transmission was associated with an increased risk of surgical site infection (8 of 73 patients [11.0%] with transmission vs 3 of 163 [1.8%] without; risk ratio, 5.95; 95% CI, 1.62-21.86; P = .007). Treatment reduced the risk of surgical site infection (hazard ratio, 0.12; 95% CI, 0.02-0.92; P = .04; with clustering by surgeon: 95% CI, 0.03-0.51; P = .004).
Conclusions and relevance: Improved basic preventive measures in the perioperative arena can reduce S aureus transmission and surgical site infections.
Trial registration: ClinicalTrials.gov Identifier: NCT03638947.
Figures
Comment in
-
Bundled Interventions to Reduce Surgical Site Infections Are Effective and Urgently Needed.JAMA Netw Open. 2020 Mar 2;3(3):e201895. doi: 10.1001/jamanetworkopen.2020.1895. JAMA Netw Open. 2020. PMID: 32219403 No abstract available.
References
-
- Boucher HW, Talbot GH, Bradley JS, et al. Bad Bugs, No Drugs: No ESKAPE! An Update from the Infectious Diseases Society of America. Clinical Infectious Diseases 2009; 48:1–12. - PubMed
-
- Vogel TR, Dombrovskiy VY, Lowry SF. Impact of Infectious Complications after Elective Surgery on Hospital Re-Admission and late Deaths in the U.S. Medicare Population. Surg Infect (Larchmt) 2012; 13: 307–1. - PubMed
-
- Awad SS, “Adherence to surgical care improvement project measures and postoperative surgical site infections”. Surgical Infection (Larchmt) 2012, 13: 234–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
