

Myocardial Infarction Can Be Safely Excluded by High-sensitivity Troponin I Testing 3 Hours After Emergency Department Presentation
- PMID: 32220124
- PMCID: PMC7496404
- DOI: 10.1111/acem.13922
Myocardial Infarction Can Be Safely Excluded by High-sensitivity Troponin I Testing 3 Hours After Emergency Department Presentation
Abstract
Background: The accuracy and speed by which acute myocardial infarction (AMI) is excluded are an important determinant of emergency department (ED) length of stay and resource utilization. While high-sensitivity troponin I (hsTnI) >99th percentile (upper reference level [URL]) represents a "rule-in" cutpoint, our purpose was to evaluate the ability of the Beckman Coulter hsTnI assay, using various level-of-quantification (LoQ) cutpoints, to rule out AMI within 3 hours of ED presentation in suspected acute coronary syndrome (ACS) patients.
Methods: This multicenter evaluation enrolled adults with >5 minutes of ACS symptoms and an electrocardiogram obtained per standard care. Exclusions were ST-segment elevation or chronic hemodialysis. After informed consent was obtained, blood samples were collected in heparin at ED admission (baseline), ≥1 to 3, ≥3 to 6, and ≥6 to 9 hours postadmission. Samples were processed and stored at -20°C within 1 hour and were tested at three independent clinical laboratories on an immunoassay system (DxI 800, Beckman Coulter). Analytic cutpoints were the URL of 17.9 ng/L and two LoQ cutpoints, defined as the 10 and 20% coefficient of variation (5.6 and 2.3 ng/L, respectively). A criterion standard MI diagnosis was adjudicated by an independent endpoint committee, blinded to hsTnI, and using the universal definition of MI.
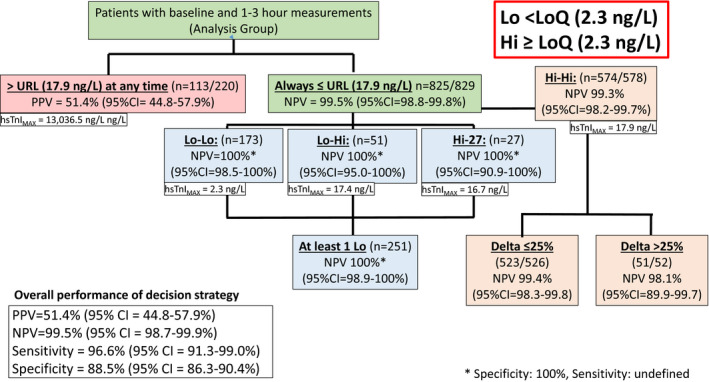
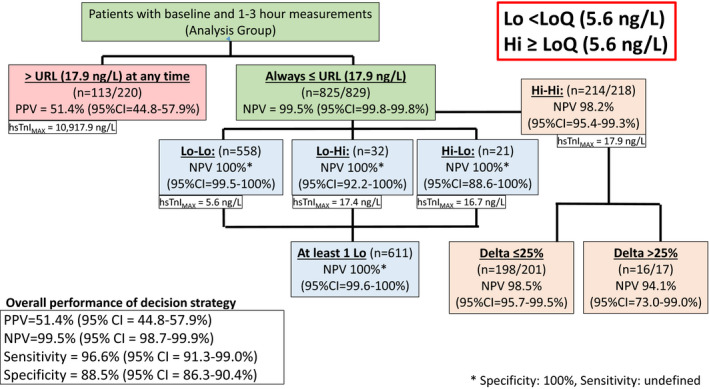
Results: Of 1,049 patients meeting the entry criteria, and with baseline and 1- to 3-hour hsTnI results, 117 (11.2%) had an adjudicated final diagnosis of AMI. AMI patients were typically older, with more cardiovascular risk factors. Median (IQR) presentation time was 4 (1.6-16.0) hours after symptom onset, although AMI patients presented ~0.5 hour earlier than non-AMI. Enrollment and first blood draw occurred at a mean of ~1 hour after arrival. To evaluate the assay's rule-out performance, patients with any hsTnI > URL were considered high risk and were excluded. The remaining population (n = 829) was divided into four LoQ relative categories: both hsTnI < LoQ (Lo-Lo cohort); first hsTnI < LoQ and 2nd > LoQ (Lo-Hi cohort); first > LoQ and second < LoQ (Hi-Lo cohort); or both > LoQ (Hi-Hi cohort). In patients with any hsTnI result <20% CV LoQ (Groups 1-3), n = 231 (23.9% ruled out), AMI negative predictive value (NPV) was 100% (95% confidence interval [CI] = 98.9% to 100%). In patients with any hsTnI below the 10% LoQ, n = 611 (58% rule out), AMI NPV was 100% (95% CI = 99.5% to 100%). Of the Hi-Hi cohort (i.e., no hsTnI below the 10% LoQ, but both < URL), there were four AMI patients, NPV was 98.2% (95% CI = 95.4% to 99.3%), and sensitivity was 96.6.
Conclusions: Patients presenting >3 hours after the onset of suspected ACS symptoms, with at least two Beckman Coulter Access hsTnI < URL and at least one of which is below either the 10 or the 20% LoQ, had a 100% NPV for AMI. Two hsTnI values 1 to 3 hours apart with both < URL, but also >LoQ had inadequate sensitivity and NPV.
© 2020 The Authors. Academic Emergency Medicine published by Wiley Periodicals, Inc. on behalf of Society for Academic Emergency Medicine (SAEM).
Figures

Comment in
-
Prognosis, Prognosis, Wherefore Art Thou Prognosis?Acad Emerg Med. 2020 Aug;27(8):783-784. doi: 10.1111/acem.14049. Epub 2020 Jul 7. Acad Emerg Med. 2020. PMID: 32542950 No abstract available.
References
-
- National Hospital Ambulatory Medical Care Survey . Emergency Department Summary Tables. 2016. Available at: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHAMC.... Accessed Aug 5, 2019.
-
- Than M, Herbert M, Flaws D, et al. What is an acceptable risk of major adverse cardiac event in chest pain patients soon after discharge from the emergency department?: a clinical survey. Int J Cardiol 2013;166:752–4. - PubMed
-
- Lyon AW, Kavsak PA, Lyon OA, Worster A, Lyon ME. Simulation models of misclassification error for single thresholds of high‐sensitivity cardiac troponin I due to assay bias and imprecision. Clin Chem 2017;63:585–92. - PubMed
-
- Jaffe AS, Apple FS, Morrow DA, Lindahl B, Katus HA. Being rational about (im)precision: a statement from the Biochemistry Subcommittee of the Joint European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation Task Force for the definition of myocardial infarction. Clin Chem 2010;56:941–3. - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation 2012;126:2020–35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
