

Whole-Exome Sequencing Analysis of the Progression from Non-Low-Grade Ductal Carcinoma In Situ to Invasive Ductal Carcinoma
- PMID: 32220886
- PMCID: PMC7367727
- DOI: 10.1158/1078-0432.CCR-19-2563
Whole-Exome Sequencing Analysis of the Progression from Non-Low-Grade Ductal Carcinoma In Situ to Invasive Ductal Carcinoma
Abstract
Purpose: Ductal carcinoma in situ (DCIS) is a nonobligate precursor of invasive breast cancer. Here, we sought to investigate the level of intralesion genetic heterogeneity in DCIS and the patterns of clonal architecture changes in the progression from DCIS to invasive disease.
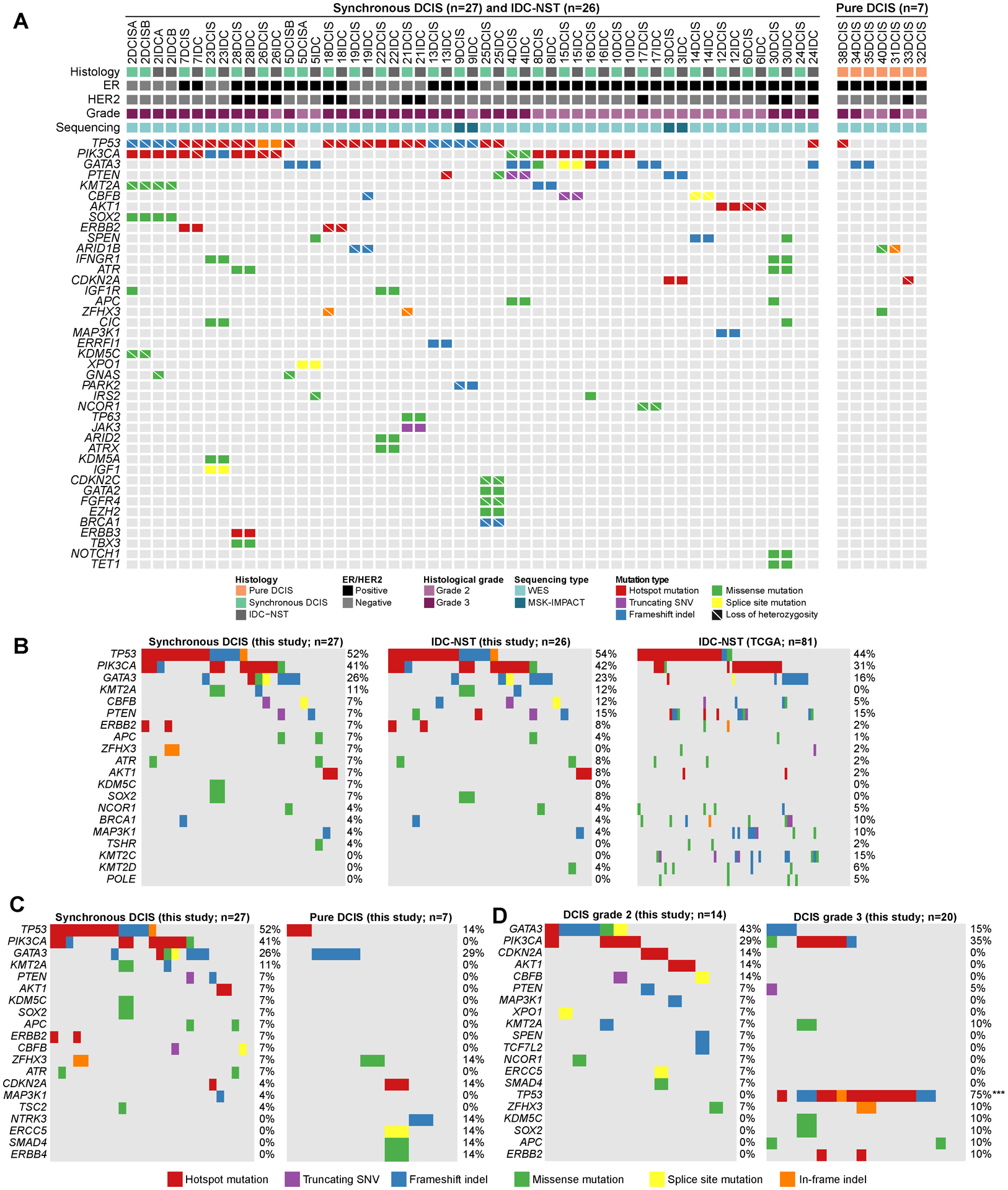
Experimental design: Synchronous DCIS (n = 27) and invasive ductal carcinomas of no special type (IDC-NSTs; n = 26) from 25 patients, and pure DCIS (n = 7) from 7 patients were microdissected separately and subjected to high-depth whole-exome (n = 56) or massively parallel sequencing targeting ≥410 key cancer-related genes (n = 4). Somatic genetic alterations, mutational signatures, clonal composition, and phylogenetic analyses were defined using validated computational methods.
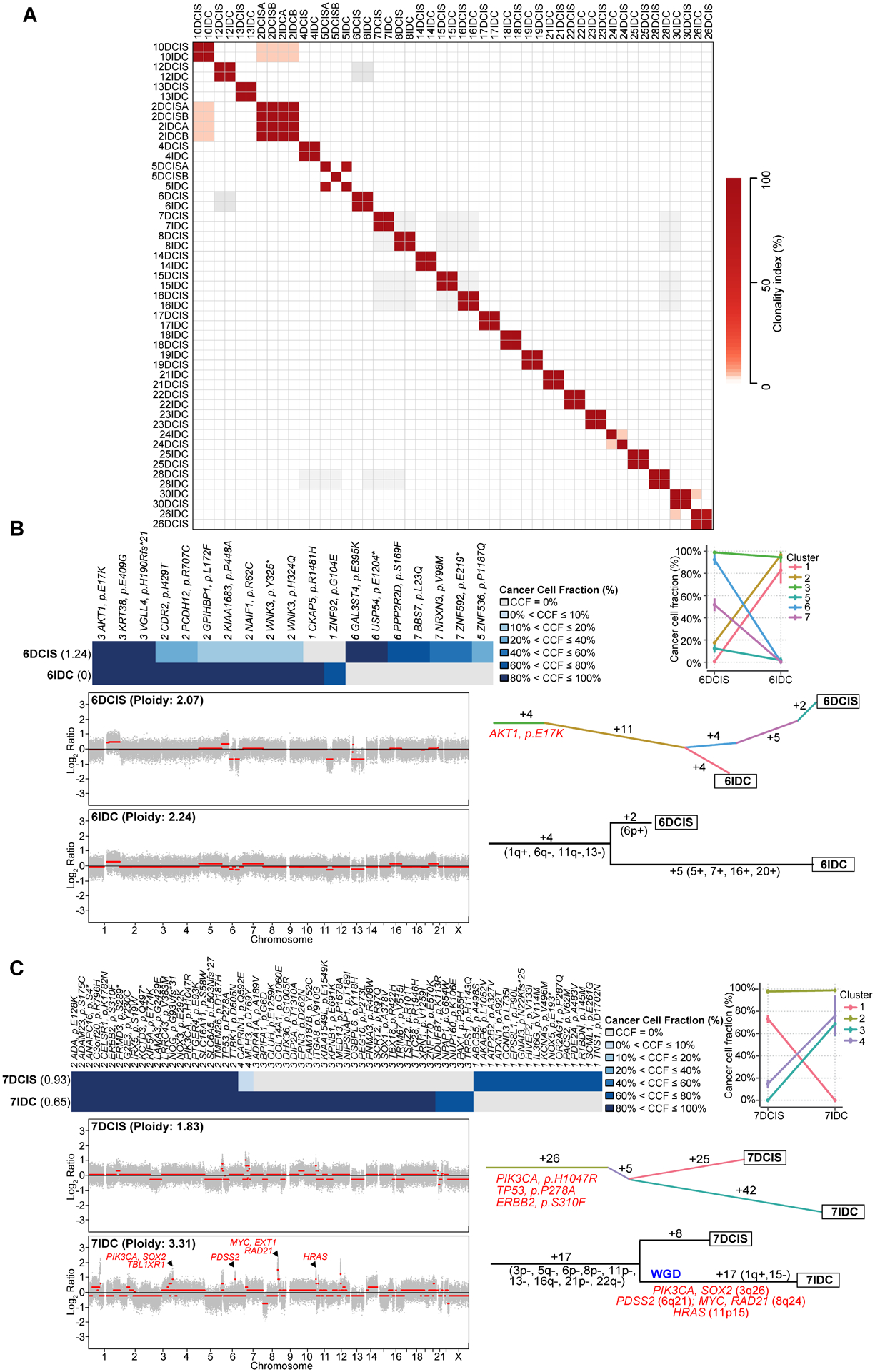
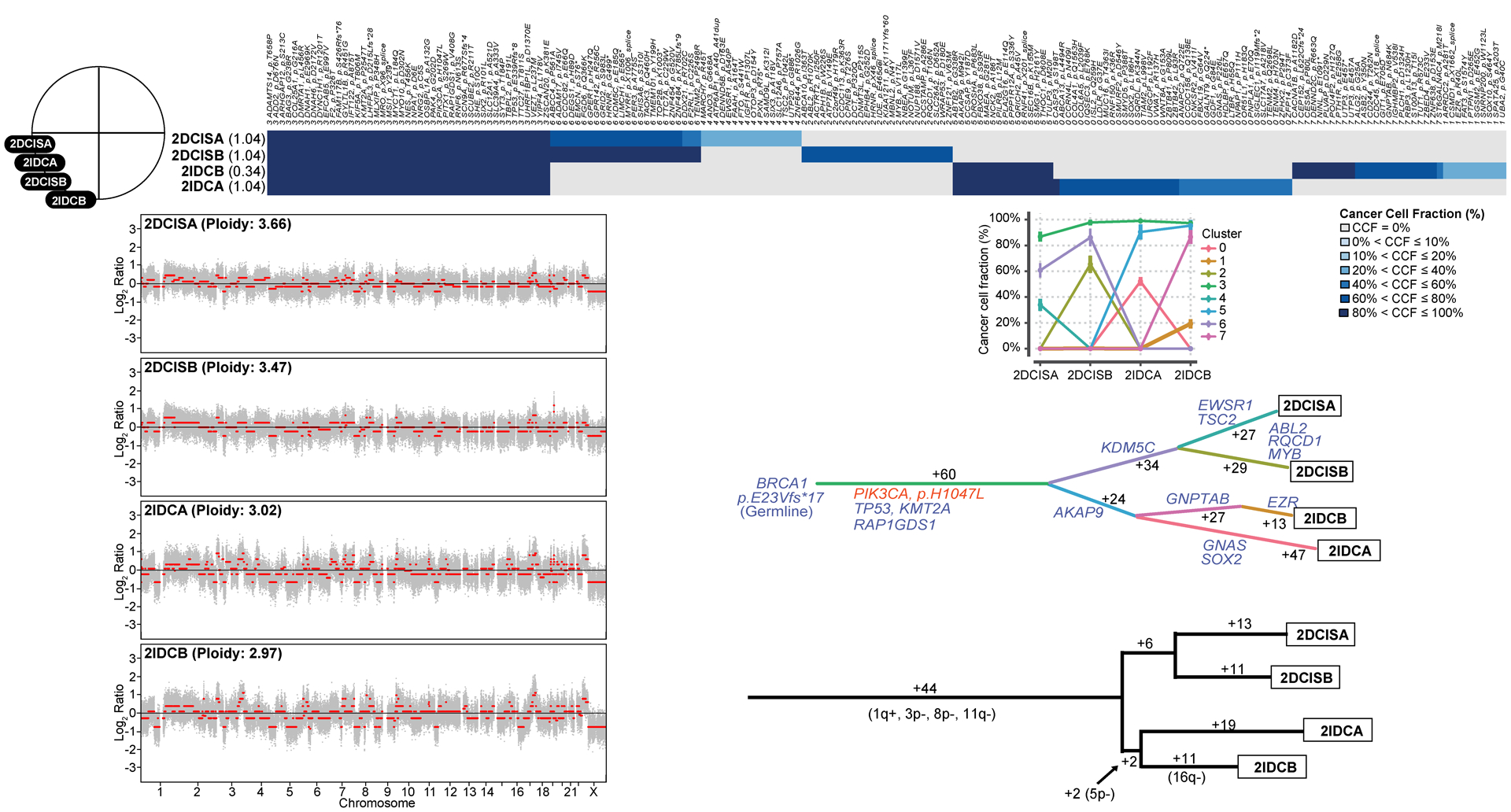
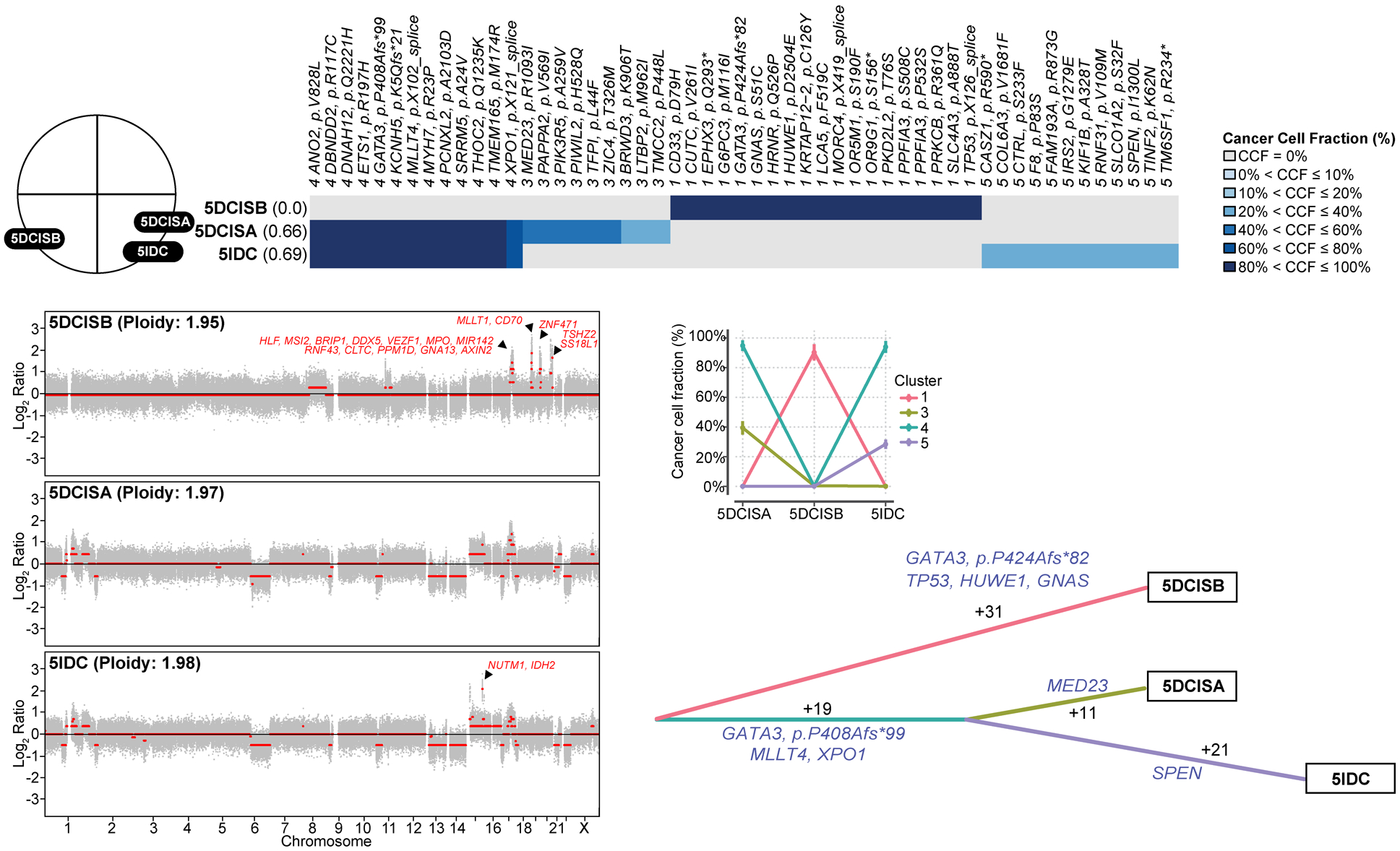
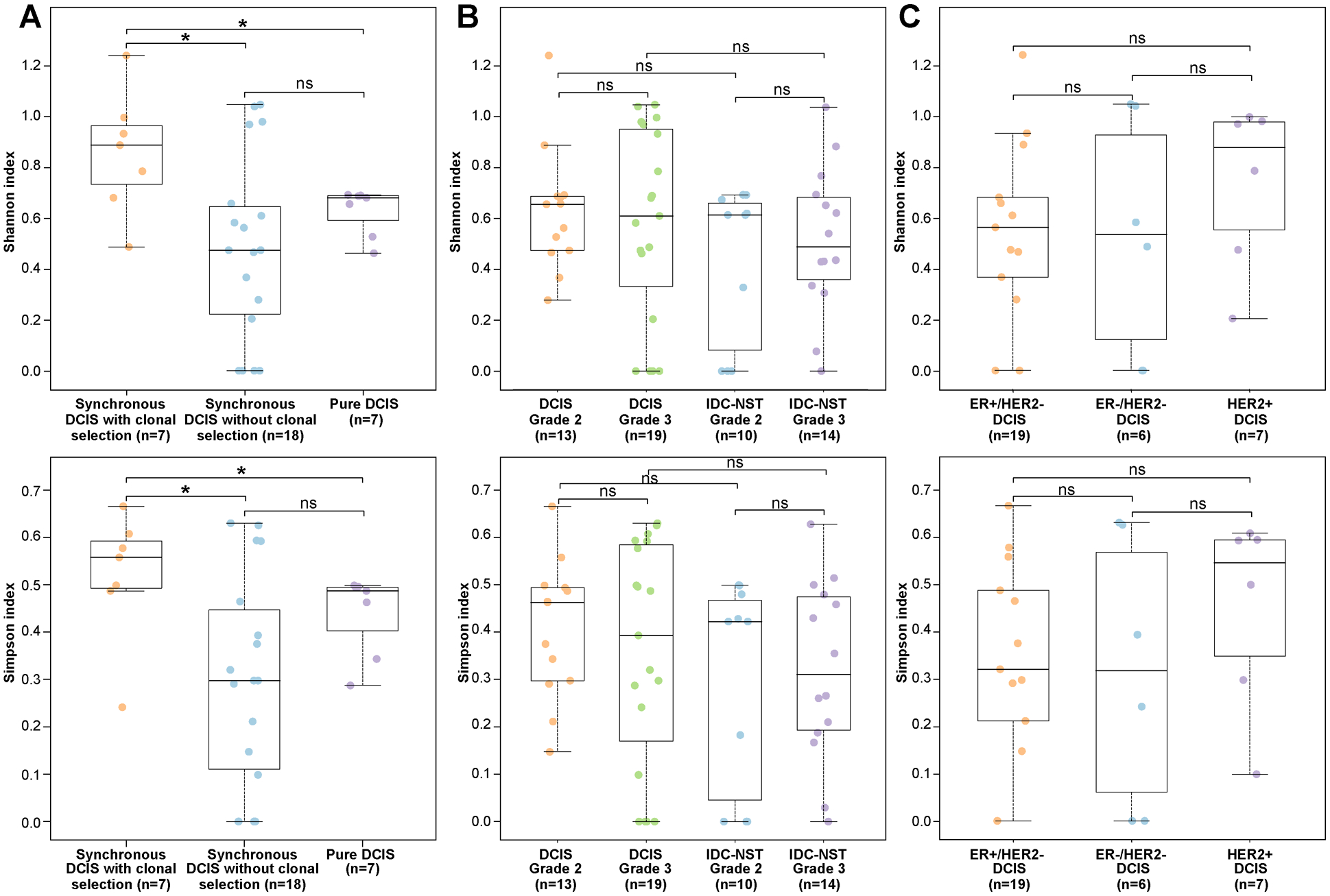
Results: DCIS revealed genetic alterations similar to those of synchronously diagnosed IDC-NSTs and of non-related IDC-NSTs from The Cancer Genome Atlas (TCGA), whereas pure DCIS lacked PIK3CA mutations. Clonal decomposition and phylogenetic analyses based on somatic mutations and copy number alterations revealed that the mechanisms of progression of DCIS to invasive carcinoma are diverse, and that clonal selection might have constituted the mechanism of progression from DCIS to invasive disease in 28% (7/25) of patients. DCIS displaying a pattern of clonal selection in the progression to invasive cancer harbored higher levels of intralesion genetic heterogeneity than DCIS where no clonal selection was observed.
Conclusions: Intralesion genetic heterogeneity is a common feature in DCIS synchronously diagnosed with IDC-NST. DCIS is a nonobligate precursor of IDC-NST, whose mechanisms of progression to invasive breast cancer are diverse and vary from case to case.
©2020 American Association for Cancer Research.
Conflict of interest statement
CONFLICTS OF INTEREST
JSR-F reports personal/consultancy fees from VolitionRx, Page.AI, Goldman Sachs, Grail, REPARE Therapeutics, Ventana Medical Systems, InVicro, Roche Diagnostics and Genentech, outside the scope of the submitted work. All other authors declare no conflicts of interest.
Figures
References
-
- Lopez-Garcia MA, Geyer FC, Lacroix-Triki M, Marchio C, Reis-Filho JS. Breast cancer precursors revisited: molecular features and progression pathways. Histopathology 2010;57(2):171–92. - PubMed
-
- Hernandez L, Wilkerson PM, Lambros MB, Campion-Flora A, Rodrigues DN, Gauthier A, et al. Genomic and mutational profiling of ductal carcinomas in situ and matched adjacent invasive breast cancers reveals intra-tumour genetic heterogeneity and clonal selection. J Pathol 2012;227(1):42–52. - PMC - PubMed
-
- Vincent-Salomon A, Lucchesi C, Gruel N, Raynal V, Pierron G, Goudefroye R, et al. Integrated genomic and transcriptomic analysis of ductal carcinoma in situ of the breast. Clin Cancer Res 2008;14(7):1956–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
