

Mapping the breast cancer metastatic cascade onto ctDNA using genetic and epigenetic clonal tracking
- PMID: 32221288
- PMCID: PMC7101390
- DOI: 10.1038/s41467-020-15047-9
Mapping the breast cancer metastatic cascade onto ctDNA using genetic and epigenetic clonal tracking
Abstract
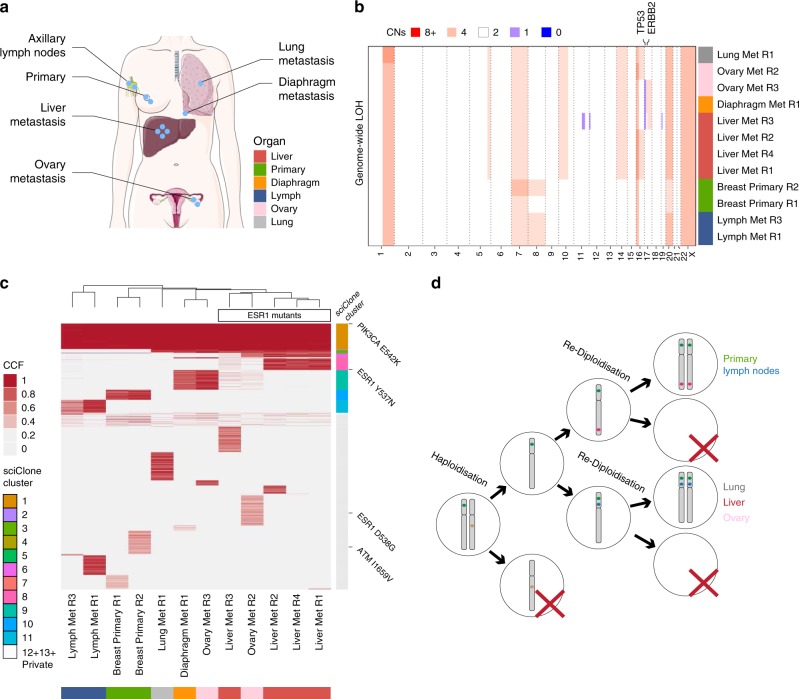
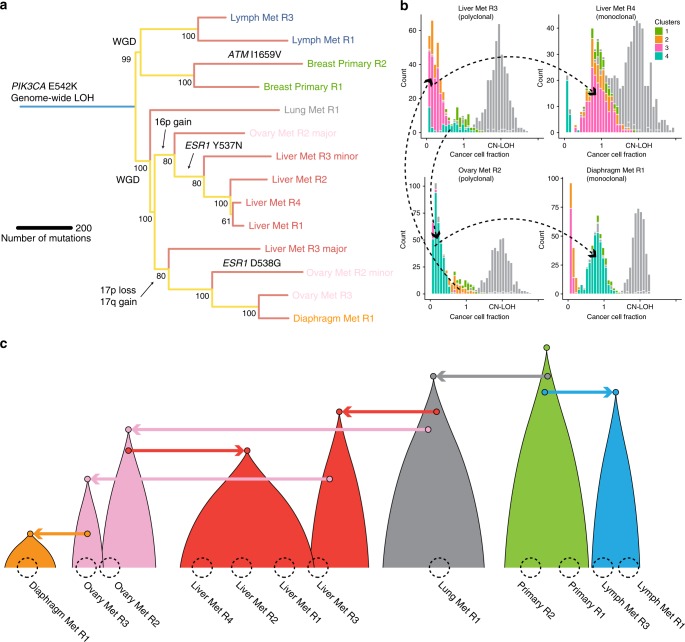
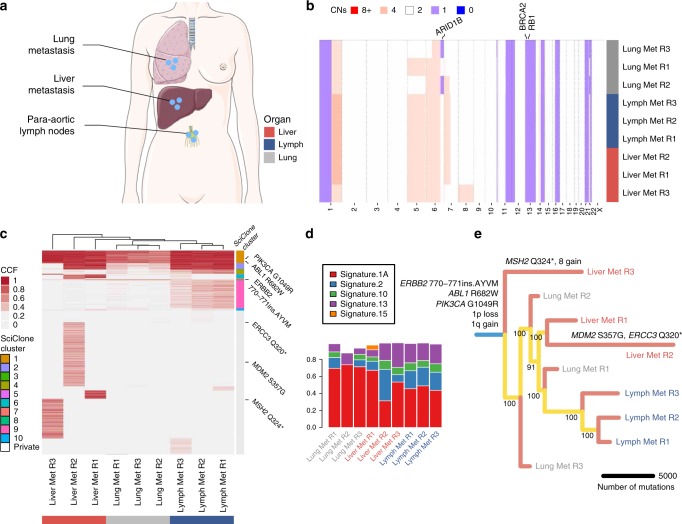
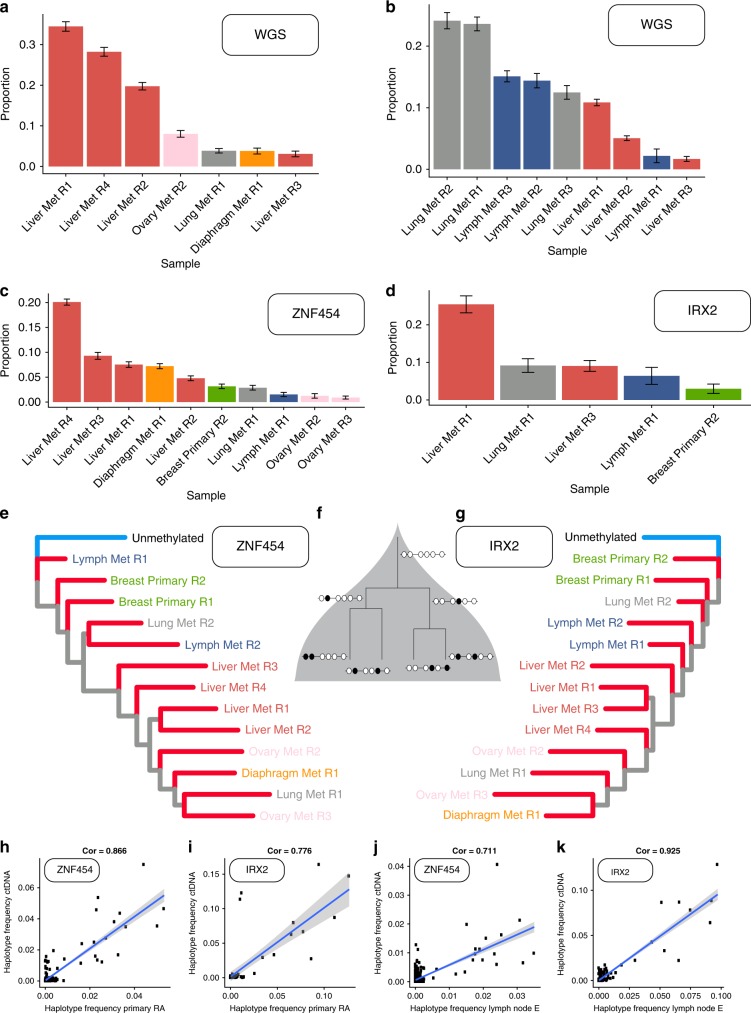
Circulating tumour DNA (ctDNA) allows tracking of the evolution of human cancers at high resolution, overcoming many limitations of tissue biopsies. However, exploiting ctDNA to determine how a patient's cancer is evolving in order to aid clinical decisions remains difficult. This is because ctDNA is a mix of fragmented alleles, and the contribution of different cancer deposits to ctDNA is largely unknown. Profiling ctDNA almost invariably requires prior knowledge of what genomic alterations to track. Here, we leverage on a rapid autopsy programme to demonstrate that unbiased genomic characterisation of several metastatic sites and concomitant ctDNA profiling at whole-genome resolution reveals the extent to which ctDNA is representative of widespread disease. We also present a methylation profiling method that allows tracking evolutionary changes in ctDNA at single-molecule resolution without prior knowledge. These results have critical implications for the use of liquid biopsies to monitor cancer evolution in humans and guide treatment.
Conflict of interest statement
G.S. is employee of AstraZeneca UK and also shareholder. A.A. is a co-founder of Tango Therapeutics, Azkarra Therapeutics, Ovibio Corporation; a consultant for SPARC, Bluestar, TopoRx, ProLynx; a member of the SAB of Genentech and GLAdiator; receives grant/research support from SPARC and AstraZeneca; A.A. holds patents on the use of PARP inhibitors held jointly with AstraZeneca which he has benefitted financially (and may do so in the future) through the ICR Rewards to Inventors Scheme.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA185138/CA/NCI NIH HHS/United States
- 105104/Z/14/Z/WT_/Wellcome Trust/United Kingdom
- 202778/B/16/Z/WT_/Wellcome Trust/United Kingdom
- P01 CA091955/CA/NCI NIH HHS/United States
- R01 CA170595/CA/NCI NIH HHS/United States
- 22909/CRUK_/Cancer Research UK/United Kingdom
- A23536/CRUK_/Cancer Research UK/United Kingdom
- 202778/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- R01 CA140657/CA/NCI NIH HHS/United States
- U54 CA217376/CA/NCI NIH HHS/United States
- A23110/CRUK_/Cancer Research UK/United Kingdom
- DH_/Department of Health/United Kingdom
- A22909/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
